A Regular SVT with Marked ST Depression
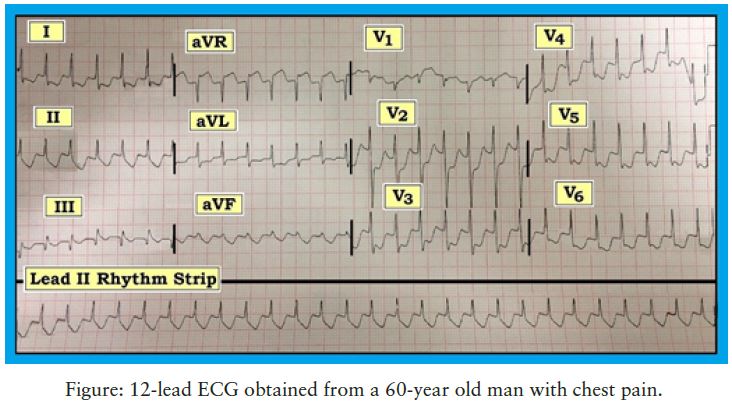
The patient is a previously healthy 60-year-old man who presented with palpitations and new-onset chest pain. He was on no medications and had no prior history of heart disease. His blood pressure was 70 systolic at the time the 12-lead ECG in the Figure 12 was obtained.
- What is the rhythm in the Figure 12?
- Why is there so much ST depression?
- What are your diagnostic considerations? Clinically, what would you do?
Interpretation: The rhythm is a regular SVT (supraventricular tachycardia) at a rate of 180/minute. The QRS complex is narrow in all 12 leads. Normal P waves are not seen.
- The principal entities to consider in the differential diagnosis of a regular SVT rhythm when normal sinus P waves are not seen are: 1.) Sinus tachycardia (with P waves hidden within the ST-T wave); 2.) Atrial flutter; and 3.) PSVT (paraoxysmal supraventricular tachycardia — also known as AVNRT = atrioventricular nodal reentrant tachycardia). Although there are other possibilities (i.e., automatic atrial or junctional tachycardias), the vast majority of regular SVT rhythms will turn out to be one of the three entities listed above.
- The rate of the SVT in this case (= 180/minute) makes it highly likely that the rhythm is PSVT. This is because sinus tachycardia is rarely this fast, and atrial flutter with 2:1 AV conduction almost always presents with a ventricular rate range between 140-160/minute.
- Perhaps the most striking finding on this tracing, however, is the marked and diffuse ST depression seen in virtually all leads (with exception of ST elevation in lead aVR).
Impression: As discussed above, the most likely etiology of this regular SVT without sinus P waves is PSVT given the rate of 180/minute. The marked and diffuse ST depression (with ST elevation in lead aVR) should prompt consideration of severe coronary disease in this 60-year-old man with new-onset chest pain. Given his low blood pressure, immediate cardioversion (rather than trial of medication) would seem warranted.
- Follow-up was available on this clinical case. The patient was not cardioverted. Instead, Adenosine was given with successful conversion to sinus rhythm. Cardiac catheterization was performed and revealed insignificant nonobstructive disease. An important lesson learned from this case is that even marked and worrisome diffuse ST depression as seen here is not always the result of severe coronary disease when the patient presents with sustained tachycardia.
Note: Further discussion of this tracing is available on an ECG video found at this site: http://tinyurl.com/nex6xc.
The patient is a previously healthy 60-year-old man who presented with palpitations and new-onset chest pain
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.