What Might Account for the ST-T Changes?
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
Dr. Grauer reports no financial relationships relevant to this field of study.
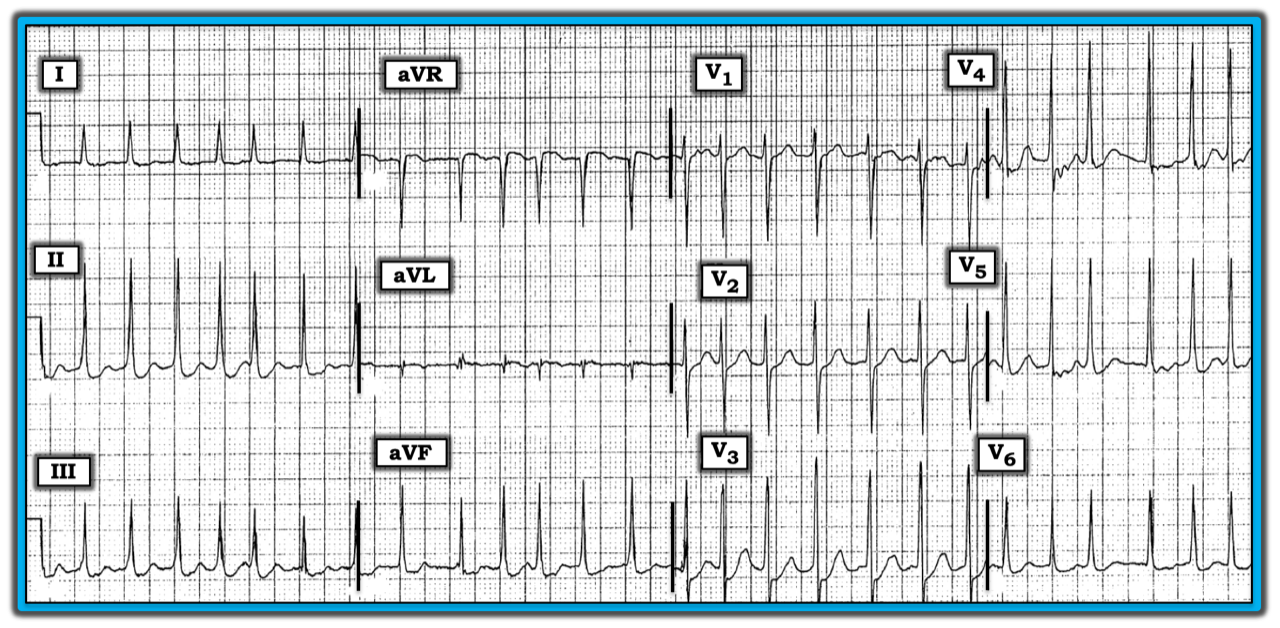
The ECG in the figure below was obtained from a 65-year-old woman who presented with an exacerbation of heart failure. A medical history revealed she was taking multiple medications. The patient was dyspneic and complained about intermittent chest pain. How might one interpret this tracing? What causes of the ST-T wave should be considered?
The rhythm is atrial fibrillation with a rapid ventricular response (irregularly irregular, without any P waves). There is no PR interval because the rhythm is atrial fibrillation. The QRS complex is narrow. The QTc is without clinical significance at this rapid rate. There is left ventricular hypertrophy (LVH), satisfied by at least two voltage criteria (deepest S wave in V1, V2 + tallest R wave in V5, V6 ≥ 35 mm, and R wave in any inferior lead ≥ 20 mm).
There are no Q waves. R wave progression is appropriate, with transition occurring between lead V2 to V3. The most remarkable finding is the “scooped” ST segment depression seen in multiple leads. There are numerous potential causes of ST-T wave depression, many of which are not cardiac-related. Among noncardiac-related causes are hyperventilation, expression of strong emotions (i.e., anxiety or fear), heat or cold exposure, neurologic disease/fatigue, nonspecific medical illness, and many others.
All that said, remember six common causes of ST-T wave depression whenever encountering the ECG finding of generalized, nonspecific ST-T wave changes. The six causes are: ischemia, repolarization changes associated with LVH (i.e., left ventricular “strain”), digitalis effect, electrolyte disorders (e.g., hypomagnesemia or hypokalemia), tachycardia, and any combination of the other five causes.
In this case, this older patient went into heart failure, experienced intermittent chest pain, was taking multiple medications, and presented in rapid atrial fibrillation. Depending on which medications she was taking (e.g., a diuretic and/or digoxin for heart failure), it may be that each cause contributed to the ST-T wave changes on this ECG.
For more information about and further discussion on this case, please visit: http://bit.ly/2kGjC0J.
The ECG in the figure was obtained from a 65-year-old woman who presented with an exacerbation of heart failure. A medical history revealed she was taking multiple medications. The patient was dyspneic and complained about intermittent chest pain.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.