ECG Review
ECG Review
A Healthy 23-year-old with a Wide Tachycardia
By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
Dr. Grauer is the sole proprietor of KG-EKG Press, and publisher of an ECG pocket brain book.
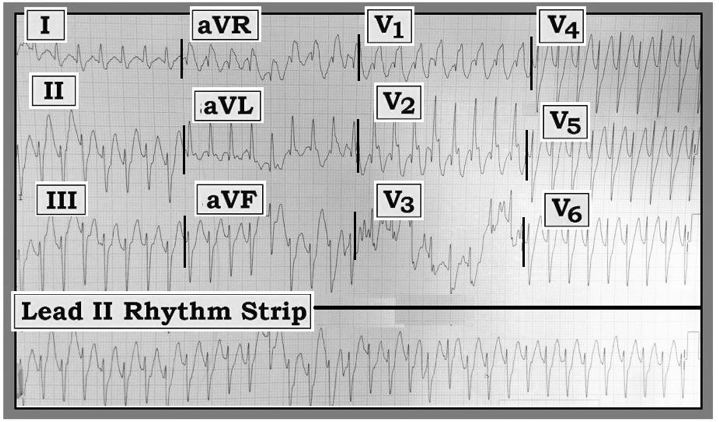
Figure — ECG obtained from a young adult with palpitations.
Scenario: Interpret the ECG and accompanying lead II rhythm strip in the Figure. The patient was a 23-year-old man who presented with "palpitations." He was presumably healthy prior to the occurrence of this arrhythmia — and he was hemodynamically stable at the time this ECG was recorded. Is the rhythm likely to be ventricular tachycardia (VT) or supraventricular tachycardia (SVT) with aberrant conduction?
Interpretation: The rhythm is a wide-complex tachycardia (WCT) without clear sign of atrial activity. Although there is some angling of the ECG paper, the rhythm appears to be regular. The rate is just over 200/minute. QRS morphology resembles the bifascicular block pattern of right bundle branch block (RBBB) with left anterior hemiBlock (LAHB).
Impression: The differential diagnosis of a regular WCT rhythm without sinus P waves should always be VT until proven otherwise. The patient should be treated accordingly. Statistically, at least 80-90% of such cases will be VT — especially if the patient is an older adult with a history of underlying heart disease. That said, there are several unique aspects to this case.
- This patient is not an "older adult with underlying heart disease." Instead, he is a healthy young adult with palpitations, but who was hemodynamically stable. Certain types of VT rhythms are known to occur in younger adults without underlying heart disease. Many of these rhythms are catecholamine-related and exercise-induced. A significant percentage of these VT rhythms (thought to account for up to 5-10% of all VT rhythms) are responsive to adenosine. This is an important reason to consider early trial of adenosine in the treatment approach to a regular WCT of uncertain etiology.
- In addition to the young age of the patient and absence of underlying heart disease, certain ECG features sometimes provide clues to the likelihood that one of these special forms of VT may be operative. This is true in this case — as the RBBB/LAHB pattern of QRS widening seen here is highly suggestive of a fascicular form of VT. QRS morphology in lead V1 is distinctly atypical for aberrant conduction — because the S wave fails to descend to the baseline and the terminal R is far wider than expected when the rhythm is SVT with aberrant conduction.
There is consensus that immediate cardioversion is indicated for treatment of a WCT rhythm whenever the patient is at all unstable. However, medical treatment with an antiarrhythmic agent is reasonable when the patient is stable, as was the case for this patient. Awareness of the existence of certain special forms of VT that are most often seen in otherwise healthy young adults can provide clues to the realization that: 1) aberrant conduction of an SVT is highly unlikely in this case; and 2) adenosine is the initial drug of choice, and may work even though the rhythm turned out to be VT.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.