ECG Review: DKA and Acute MI?
By Ken Grauer, MD
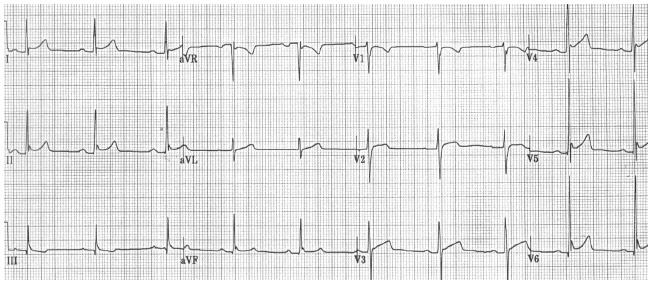
Figure. 12-lead ECG obtained from a 32-year-old man who presented in DKA.
Clinical Scenario: The ECG in the Figure was obtained from a previously healthy 32-year-old African American male who presented in a coma from diabetic ketoacidosis (DKA). Cardiovascular exam was unremarkable. In addition to being treated for DKA, should he also be considered a potential candidate for thrombolytic therapy?
Interpretation: The ECG in the Figure shows normal sinus rhythm at a rate of about 60/minute. The PR interval is at the upper range of normal ( = 0.21 second). The QRS and QT intervals are normal. The mean QRS axis is +60°. In view of the patient’s age, there is no evidence of chamber enlargement. Perhaps the most remarkable finding on this tracing is the presence of diffuse ST segment elevation. This finding is present in virtually all leads except III, aVR, and V1. It is most marked in lead V5, where ST segment elevation attains at least 3 mm.
Despite the presence of diffuse ST elevation, it is highly unlikely that this pattern represents acute infarction. ST segment morphology is clearly upsloping (upward concavity), with marked notching of the J point in multiple leads (especially II, V4, V5, and V6). The ST segment appearance that is characteristic of acute infarction is more typically coved (downward convexity) and usually is localized to one or two specific lead areas, rather than being as generalized as it is here. Marked acute ST segment elevation indicative of acute infarction also commonly is associated with reciprocal ST segment depression, which is not seen here. Although Q waves are present in the inferolateral leads, they are quite small and narrow. This is much more consistent with normal septal Q waves rather than acute evolving infarction. Clearly, clinical correlation is needed. However, given the young age of this patient, his negative past medical history, the apparent absence of chest pain, and the ECG picture described above, early repolarization almost is certain to be the cause of diffuse ST elevation in this case.
The shape of ST segment elevation provides a key clue to its etiology in this case (upsloping in multiple leads with prominent J-point notching). Admittedly, acute pericarditis at times can produce diffuse ST elevation similar to that seen here. However, the history in this case does not suggest acute pericarditis, tachycardia is absent, no mention of a pericardial friction rub is made, and the ECG picture with prominent J-point notching seen here is much more suggestive of early repolarization.
Dr. Grauer, Professor and Associate Director, Family Practice Residency Program, Department of Community Health and Family Medicine, College of Medicine, University of Florida, Gainesville, is on the Editorial Board of Emergency Medicine Alert.
The ECG in the Figure was obtained from a previously healthy 32-year-old African American male who presented in a coma from diabetic ketoacidosis (DKA). Cardiovascular exam was unremarkable. In addition to being treated for DKA, should he also be considered a potential candidate for thrombolytic therapy?
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.