Dodging the Bullet: Part II
Dodging the Bullet: Part II
A review and discussion of several close clinical encounters
By Adrian Amin, MD, Senior Resident, Department of Emergency Medicine, Medical College of Georgia, Augusta, and Larry Mellick, MD, MS, FAAP, FACEP, Professor of Emergency Medicine and Pediatrics, Department of Emergency Medicine, Medical College of Georgia, Augusta
The first “Dodging the Bullet” article was written and published in the September 2011 issue of ED Legal Letter. In the earlier article, as well as this article, a series of actual clinical cases are presented that could have turned out differently if the wrong management decision had been made. The goals of this article remain the same as the earlier one: to glean important points of educational and teaching value from each of the reported high risk cases; and to highlight the fact that clinical misadventures are often a single judgment call away from a potential tragedy. I am confident that every emergency medicine physician practicing could write their own case series of near misses. That’s simply the nature and reality of practicing medicine in the emergency department. And, as stated previously, our decision-making processes are often complicated, tenuous, and treacherous at times, and, consequently, the odds are not in our favor. Therefore, as stated previously, it is just a matter of time before the bullet finds its mark, and we can only hope that “harm is minimized, our documentation supports our decision making, and that the patient and his or her family are understanding and forgiving.”
Nebulous Nasal Congestion
An elderly man presented to the emergency department with complaints of nasal congestion. He had no difficulty breathing orally, but his lack of ability to breathe nasally was causing him concern. Upon examination, he had a systolic blood pressure of 93 mm Hg and a heart rate of 110 bpm. The patient was questioned regarding his low blood pressure, and he stated that his blood pressure often fell at the lower end of normal. Upon review of available past records, his blood pressure was indeed found to be in alignment with previous findings.
Figure 1: Patient with nasal congestion
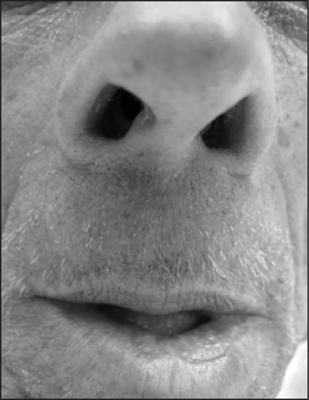
The patient’s known medical conditions were metastatic squamous cell carcinoma and asthma; however, at the time of presentation, he said he “felt fine.” His physical examination was unremarkable. Upon gentle probing for additional symptoms, the patient mentioned a tendency to be claustrophobic and offered that his current symptoms might be explained by his anxiety.
Because the presentation was benign, preparations were begun for his discharge. However, after a last-minute discussion between the attending physician and resident, a decision was made to order a complete blood count (CBC). These test results demonstrated a WBC count of 26,000/mm,3 along with a 3-gram drop in hemoglobin (7.5 g/dL). (See Figure 2.) A chest X-ray was ordered, which showed a large lung abscess. (See Figure 3.) The patient was started on piperacillin/tazobactam and vancomycin. Within a few hours of presentation, the patient’s condition deteriorated and his systolic blood pressure dropped into the 60s and his heart rate increased to 130. He was promptly admitted into the MICU.
Figure 2: Laboratory testing showing an elevated white count and low hemoglobin 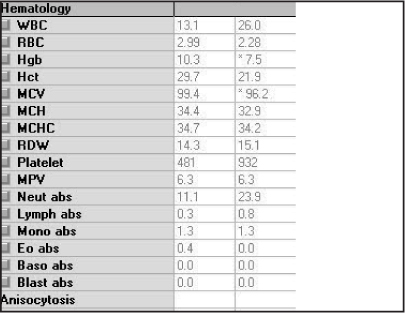 |
Figure 3: Chest X-ray demonstrating large lung abscess 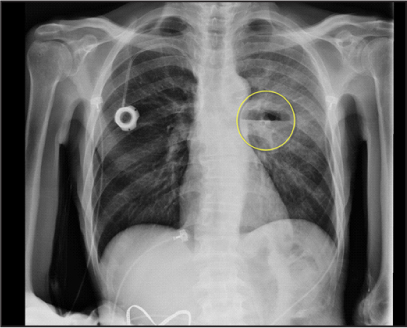 |
A chest radiograph demonstrated a 6 cm cavitary lesion that involved the superior segment of the left lower lobe, with air fluid level and surrounding airspace consolidation. Given its rapidity of development, this finding was consistent with necrotizing pneumonia. It was uncertain whether there was fistulous communication with the esophagus or adjacent bronchus. No additional pulmonary lesions were demonstrated, and there was a very small pleural fluid component evident.
Following admission, the abscess was drained using CT guidance. Manual aspiration yielded approximately 10 mL of frank pus. The tract was serially dilated and a 12 French drainage catheter was placed over the guide wire into the left upper lung abscess. The catheter was placed to waterseal and secured at the skin entry site with a silk suture. No complications occurred.
Discussion
Emergency medicine physicians are often faced with seemingly insignificant symptoms that, on the surface, can appear to be unrelated. However, it is the clinical judgment and perhaps an unexplainable feeling or concern that may prompt physicians to dig deeper to ensure different aspects are considered. In many cases, it may be helpful to consider alternate options besides the obvious to determine if there really is a medical concern. In this case, the last-minute decision to perform a CBC was integral to finding and draining a deepseated, pus-filled abscess that had the potential to lead to an undesirable outcome.
Learning Points
• Never completely trust your own clinical judgment and diagnostic acumen.
• For vulnerable patients who are not overtly symptomatic, it is sometimes better to err on the side of caution and consider performing further testing or a diagnostic procedure to detect an underlying condition.
Hidden from View: Tibial Plateau Fracture
An adult male was transferred from an outside hospital for the evaluation of possible compartment syndrome after having his legs caught between several large trees that fell. His diagnosis was negative for compartment syndrome; however, he continued to have a painful gait, with the pain mostly in the posterior calf with ambulation. On palpation, he was tender on the medial and lateral proximal right tibia. (See Figure 4.) His plain films, including oblique views, showed no apparent fracture. (See Figure 5.) In a recent morbidity and mortality conference, there was a discussion of a similar case of a missed tibial fracture that was not visible on X-ray but was apparent on CT scan. Simply because there was a significant degree of similarity between the two cases, a CT scan was ordered of the proximal tibia. To our surprise, the CT scan demonstrated a tibial plateau fracture. (See Figure 6.) The patient’s leg was splinted in the emergency department, and the fracture was subsequently treated by the orthopedic department by internal fixator placement and immobilization via a long leg splint. (See Figure 7.)
Figure 4: Swollen, tender calf with evidence of bruising  |
Figure 5: Plain films of the knee that appear to be normal  |
Figure 6: CT scan demonstrating evidence of tibial plateau fracture  |
Figure 7: Splinting the fracture in the emergency department  |
Discussion
Most fractures of the tibial plateau are readily diagnosed by conventional radiography. However, as in the case above, in the event that unremarkable findings are present in traditional radiography films, a CT scan should be considered to gain a clearer view of the articular surface of the tibia.
CT scans provide reconstruction of axial images into coronal and sagittal planes, which allow for localization of surgical landmarks as well as fracture fragments. Since CT scans are generally able to depict all fractures, it is important that both coronal and sagittal reconstructions of axial data are incorporated to avoid false-negative errors that can occur when only axial imaging is used. For example, if a fracture predominates in the axial plane, it may be overlooked in the CT, leading to inaccurate diagnosis and subsequent treatment. Through the reconstruction of data into different planes, additional information such as articular depression and diastasis may be obtained easily.
Learning points
• Morbidity and mortality meetings allow physicians to learn from the clinical misadventures of others and enhance diagnostic acumen in seemingly cut-and-dry cases.
• In the event that traditional radiologic films show unremarkable results and the patient’s findings are more consistent with a fracture, consider using more evolved technology such as CT scans to gain both coronal and sagittal planes for more detailed imaging of possible fracture sites.
Oral Cancer
For a second time in a week, a 55-year-old male presented to the emergency department for evaluation of tooth pain. He had been followed by a dentist for about six weeks, and the dentist had even pulled a tooth suspected of being the cause of the pain. (See Figure 8.) During the first emergency department visit, the patient was treated with pain medications and antibiotics for a suspected abscessed tooth and discharged home.
Figure 8: Previously extracted tooth carried by the patient’s wife

During the second emergency department visit, the resident who first evaluated the patient expressed concern that the patient was exhibiting drug-seeking behavior. However, a second and closer look revealed an ulcerated tongue lesion. (See Figure 9.)
Figure 9: Ulcerated tongue lesion due to oral cancer
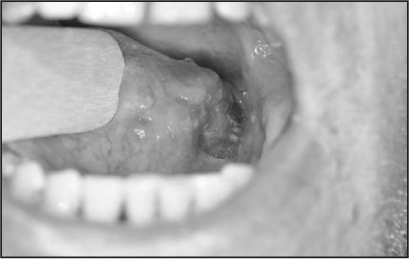
The patient thought a sharp tooth was ulcerating his tongue and causing constant pain. However, the patient reported a 20-pack-per-year history of smoking and daily alcohol consumption. A CT scan with contrast showed a lesion consistent with cancer of the tongue.
Otolaryngology (ENT) was consulted. The ENT team biopsied the lesion and arranged follow up. The patient subsequently underwent extensive surgery of the tongue and neck for squamous cell carcinoma of the left tongue and tonsil.
Discussion
Squamous cell carcinoma is the most common malignancy of the tongue. There are three growth patterns recognized, which include the ulcerative type seen in our patient. Tobacco use is strongly associated with oral cavity cancers, and tobacco use is documented in up to 90% of patients with oral cavity cancers. Alcohol consumption is also strongly associated with oral cavity cancers.
The bullet was dodged because the physicians did not anchor too early on the diagnosis. Early anchoring on a diagnosis is one of the reasons diagnostic misadventures occur.
Nevertheless, six weeks of dental evaluations, an unnecessarily extracted tooth, and two visits to the emergency department took place before the diagnosis was made.
A YouTube video of this patient’s presentation can be seen at the following link: http://www.youtube.com/watch?v=GBDcnjN4TN0.
Learning Points
• Premature closure on the wrong diagnosis is a common cause of misdiagnosis in the practice of medicine.
• While drug-seeking behavior is commonly seen in the emergency department, it is critical that emergency physicians avoid becoming overly suspicious of patients who return for evaluation of painful conditions.
Every patient deserves a thorough evaluation of their complaint, no matter how frustrating their behavior or their frequency of visits to the emergency department.
The Diagnostic Challenge of Newborns
An 11-day-old infant was brought to the emergency deparment and presented with loose stools. The first-time mother stated that the baby “felt warm,” but there was no other documentation of fever. Upon examination, the baby was vigorous, feeding appropriately, and afebrile with normal vital signs. The number of loose stools was consistent with normal newborn patterns. The patient was discharged. The attending physician instructed the mother to check the infant’s temperature with a thermometer and to return if the temperature was greater than 100.4°F. Two days later, the infant returned to the emergency department with a fever. A septic work-up was initiated, but venous access was difficult.
Multiple intravenous (IV) line attempts resulted in only enough blood for a CBC and blood culture. A decision was made to proceed with a CSF tap, with plans to administer antibiotics intramuscularly immediately afterward. The results of the CSF were as follows: color: straw; clarity: slightly hazy; WBC: 1,025/mm3; RBC: 28/mm3; WBC differential: segmented neutrophils 28%; lymphocytes 49%, and monocytes 23%; protein: 236 mg/dL; glucose: 43 mg/dL; the Gram stain was negative. (See Figure 10.) However, the culture of the cerebrospinal fluid subsequently demonstrated growth of “rare Listeria monocytogenes.”
Figure 10: Cloudy spinal fluid
Discussion
Listeria monocytogenes is a ubiquitous gram-positive, motile, rod-shaped bacterium. The principal route of acquisition of Listeria is through the ingestion of contaminated food products. It is not uncommon for pregnant women to carry Listeria asymptomatically in their GI tract or vagina. These maternal Listeria infections can result in chorioamnionitis, premature labor, spontaneous abortion, or stillbirth. Fetal infection can occur via transplacental transmission, but vertical transmission can also occur from mother to infant during passage through an infected birth canal. There are two clinical presentations of neonatal infections: early onset (< 5 days) and late onset (> 5 days). Early-onset neonatal listeriosis is usually associated with sepsis or meningitis. As was found with our patient, late-onset Listeria neonatal infections frequently present as life-threatening purulent meningitis.
The primary reason for performing a lumbar puncture on a febrile infant or child is to differentiate viral meningitis from bacterial meningitis. While viral meningitis significantly outnumbers bacterial meningitis by as much as 50:1, bacterial meningitis is significantly more common in newborns, hence the strong recommendation of a full sepsis work-up in febrile infants younger than 1 month of age.
In the event there is a limited amount of sample to perform laboratory tests, it is recommended to perform a Gram stain and culture, as Gram stains from bacterial meningitis are positive in approximately 70% of cases.
An important note to mention in this case is that the mother telephoned the pediatric emergency department requesting advice from a physician about her child. The emergency department clerk was overheard advising the patient’s mother to contact her pediatrician. After hanging up, the clerk’s response was, “Their 13-day-old baby had a fever and I told the mother to call their pediatrician.” The temptation of non-medical personnel to give advice over the telephone is a recurrent issue, and in this case, could have delayed the return of this infant to the emergency department. Thankfully, this did not happen, and the child was brought to the emergency department in a timely manner.
Learning Points
Even though giving advice over the telephone is generally discouraged, there are certain situations when advice should be given. In this case, an urgent request to bring a febrile neonate in for an emergent evaluation was mandatory to prevent any untoward outcomes.
Don’t allow procedures to delay life-saving treatment. While it was difficult to obtain intravenous access on this infant, the precedence of performing a cerebrospinal fluid (CSF) tap and administering antibiotics was more important than continuing to attempt IV access.
Never underestimate the subtle presentations of sepsis in neonates. The patient was seen in the emergency department two days previously with signs of infection: felt warm, was spitting up, and had a change in stool pattern. Subtle, nonspecific, early signs such as these need to be rapidly evaluated in these young patients.
Deep Venous Thrombosis
A 61-year-old male presented to the emergency department for evaluation of posterior left knee pain that had been present for one week. The patient admitted to an event of mild trauma when he hit the knee on a step while bending it. As a construction worker, he described walking up and down stairs frequently. He also described the pain as predominantly on the posterior aspect of the left knee, with radiation of pain down the back of the calf. He also reported tingling and numbness.
The examination demonstrated a nearly normal examination of the left lower extremity. There was no swelling, erythema, or ecchymosis. (See Figure 11.) The only positive finding was tenderness with palpation of the left posterior medial knee.
Figure 11: Relatively normal- appearing lower extremities despite a large DVT clot load

Both the physician assistant and attending physician were suspicious that the patient’s pain was caused by a Baker’s cyst. An ultrasound of the left lower extremity was obtained to assess for the presence of a Baker’s cyst. The possibility of a deep vein thrombosis was considered, but physical evidence for a deep vein thrombosis was nearly non-existent. Nevertheless, multiple color Doppler and grayscale images of the left lower extremity demonstrated extensive acute deep vein thrombosis within the left lower extremity. Acute deep vein thrombosis was noted in the superficial femoral, greater saphenous, popliteal, gastrocnemius, and lesser saphenous veins. The patient was treated as an outpatient with Lovenox® (enoxaparin sodium injection), and follow-up was arranged.
Discussion
The bullet dodged with this patient was an examination and history more consistent with a medical condition other than the life-threatening condition discovered. Deep vein thrombosis can be subtle in its presentation, and this patient had no risk factors except a vague history of trauma. Nevertheless, a failure to make the diagnosis of deep venous thrombosis in the patient could have resulted in a fatal outcome for this patient.
Learning Points
• Even though the practice of medicine has zero tolerance for diagnostic failures, and delays in diagnosising the complexity and variability of disease presentations make perfection impossible. Consequently, it is important to educate our patients that disease presentations are rarely classic and disease progression is sometimes required before a condition can be diagnosed.
Summary
This article highlighted a number of clinical scenarios in which misdiagnoses were barely averted. The goal is to help others avoid the similar near misses and traps in clinical decision making. Additionally, the authors hope to emphasize the uncontrolled environment and potential risks that occur when large numbers of undifferentiated patients present to the emergency department for evaluation.
Because physicians are humans prone to error, and disease processes frequently do not fit the classic description, clinical perfection is not always possible. Thankfully, most delays in diagnosis and timely management do not have serious consequences. When they do, however, it is important to have documented the findings and thought processes well and to have maintained a positive relationship with the patient and his or her family.
The first Dodging the Bullet article was written and published in the September 2011 issue of ED Legal Letter. In the earlier article, as well as this article, a series of actual clinical cases are presented that could have turned out differently if the wrong management decision had been made. The goals of this article remain the same as the earlier one: to glean important points of educational and teaching value from each of the reported high risk cases; and to highlight the fact that clinical misadventures are often a single judgment call away from a potential tragedy.Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.