ECG Review: A Helpful Hand from aVR
ECG Review
A Helpful Hand from aVR
By Ken Grauer, MD, Professor Emeritus in Family Medicine, College of Medicine, University of Florida. Dr. Grauer is the sole proprietor of KG-EKG Press, and publisher of an ECG pocket brain book.
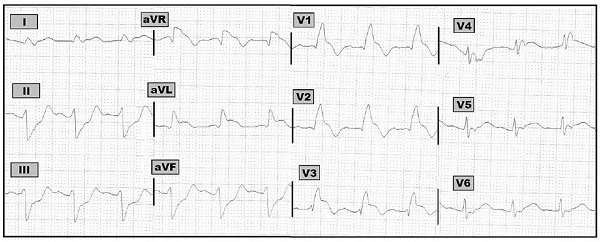
Figure 12-lead ECG obtained from a patient with new-onset chest pain.
Scenario: The 12-lead ECG shown above was obtained from a patient with new-onset chest pain. Where is the acute lesion likely to be?
Interpretation: The rhythm is sinus tachycardia at about 100/minute. The PR interval is relatively long given the fast rate (though not quite satisfying criteria for 1st degree AV block). The QRS complex is wide in the pattern of right bundle branch block (RBBB). There is marked left axis deviation consistent with left anterior hemiblock which makes the conduction defect at least a bifascicular block. There are small q waves in leads aVL, V1, and V2, with the most remarkable finding being the marked ST elevation in multiple leads (including leads I, aVR, aVL, and V1-through-V6). In addition, there is reciprocal ST depression in each of the inferior leads. Obviously, extensive myocardial infarction is acutely ongoing. Specifically, there very likely is acute occlusion of the left main coronary artery. This is an indication for urgent cardiac catheterization.
This tracing provides an excellent example of one of the very few instances when lead aVR may prove highly insightful. Most of the time, the remote right-sided and superior lead location of aVR provides little clinically useful information beyond suggesting on rare occasions that there may be lead misplacement or dextrocardia. It is helpful to be aware of two additional situations in which recognition of ST elevation in lead aVR may be instructive: 1) in the presence of diffuse ST depression, the finding of ST elevation in lead aVR suggests the patient has either three-vessel or left main coronary artery disease; and 2) in patients with acute coronary syndrome who have acute left main coronary artery occlusion. The findings in the Figure are highly suggestive of the latter situation. This is because the patient has new-onset chest pain; there is marked and diffuse ST segment elevation in multiple leads with reciprocal ST depression in the remaining leads; there is significant conduction system disease including RBBB (which is highly characteristic of acute left main occlusion); and there is more than 1 mm of ST elevation in lead aVR.
The 12-lead ECG shown above was obtained from a patient with new-onset chest pain. Where is the acute lesion likely to be?Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.