Evaluation and Management of Traumatic Wounds
Authors
David A. Notley, MD, Clinical Instructor of Emergency Medicine, Ohio State University, Columbus.
Daniel R. Martin, MD, Professor and Vice Chair of Education, Department of Emergency Medicine, Ohio State University, Columbus.
Maxwell Hill, MD, Assistant Professor of Emergency Medicine, Assistant Program Director, Ohio State University, Columbus.
Peer Reviewer
Dennis Hanlon, MD, Vice Chairman of Emergency Medicine, Associate Professor of Emergency Medicine, Allegheny General Hospital, Pittsburgh, PA.
Traumatic wounds are a common cause of ED visits and are often managed exclusively by the emergency medicine provider. Most of these patients are evaluated, appropriately treated, and discharged with satisfactory outcomes. Although outcomes are similar, there are no specific preferred treatments for traumatic wound injuries, and this requires the emergency provider to develop comprehensive efficacy strategies on how to approach these common injuries. Wound closure materials, techniques, and management strategies vary widely, with both the preferences of the physician and the patient influencing the final decisions.
— Ann M. Dietrich, MD, Editor
The general approach to wound management in the ED is as follows: stop the bleeding, prevent infection, and maximize both functional and cosmetic outcomes. The most appropriate way to accomplish these tasks is still up for debate. Methods of wound irrigation, pain control, sedation, and even the timing of wound closure are topics that are not clearly defined in the medical literature. For some topics, such as antibiotic use, the medical literature and emergency department common practice are often at odds, making the topic confusing for practitioners.
This article reviews specific methods and approaches to traumatic wound repair. The goal is an evidence-based practical guide for emergency medicine clinicians, which may serve as a basis for simple practice adjustments or for implementation of entirely new techniques in a clinician’s acute wound care management.
Introduction
Traumatic wounds are a major cause of emergency department visits in the United States. Between 1992 and 2002, there were more than 90 million lacerations treated in U.S. emergency departments.1 The ultimate goals of therapy, in relative order of importance, include prevention of infection, maintenance of function, optimal cosmetics, and reduction in periprocedural discomfort. These goals are accomplished with appropriate planning, preparation, procedural technique, and patient education.
Wounds are not only a major source of ED visits each year, they are also a common source of patient dissatisfaction, complaints, and, not surprisingly, malpractice cases. In one analysis, approximately 20% of malpractice cases were related to issues and complications with wound management.2,3 In the majority of these cases, the main complaints were missed foreign body, missed tendon injury, or missed nerve injury.2 Correct evaluation, technique, and procedural approach to emergency wound care are essential in avoiding these and other complications.
Wound Anatomy and Physiology
There are four layers of tissue that require evaluation and possible repair in the setting of an acute traumatic wound. From superficial to deep, these layers are the epidermis, dermis, subcutaneous layer, and deep fascia. Each of these layers has specific qualities that must be addressed during wound repair.
The epidermis is the key cosmetic layer and should be manipulated with care. Caution should be used when grasping this tissue, and is best achieved with gentle use of specific tissue forceps, which have sharp, “rat-tooth” jaws that minimize crushing of tissue. The dermis is the key layer for tensile strength and is the layer that suture must penetrate and secure for appropriate wound closure. The subcutaneous tissue contains blood vessels and nerves, and as such must be handled with care during repair, and is a key layer for anesthesia. The deep fascia, beneath the subcutaneous tissue should be considered for closure if violated and may require a surgical evaluation if there is concern for inadequate wound closure, or if there is suspicion of injury to critical structures, including tendons, nerves, and deeper blood vessels.
A knowledge of the mechanism of injury will not only aid the clinician in appropriate wound management, but will also allow for better counseling of the patient in regard to wound healing and potential complications. Table 1 shows various types of force, damage generated, and general outcome for traumatic wounds often encountered in the emergency department.
Table 1. Types of Traumatic Wounds
|
Type of Force |
Cause |
Extent of |
General |
|
Shearing force |
Sharp object — knife, glass |
Little adjacent damage |
Heals well |
|
Avulsion (tension) |
Blunt object, acute angle |
Moderate cell disruption causing tissue flap |
Heals poorly |
|
Compression (crush) |
Blunt object, right angle |
Cell destruction |
Heals poorly, high infection risk |
Once the mechanism of injury has been determined, and the extent of injury assessed, specific techniques for wound closure can be addressed with the goal of optimizing healing and functionality. Managing patient expectations throughout the assessment and repair, and involving the patient in wound care decisions with associated patient education on the process of wound healing, can maximize patient satisfaction and prevent unnecessary concern over normal healing processes.
Wound healing is complex and occurs in stages. Immediately post-injury, the tissue responds by contracting, the vessels constrict, and coagulation begins, leading to hemostasis. In the absence of inhibiting or aggravating factors, this process lasts approximately 6 hours. The inflammatory phase begins at approximately 6 hours; cytokines and other chemical mediators are released, which attract lymphocytes, granulocytes, and other inflammatory cells to the area. The numbers of these cells peak at about 24 hours. Around this time, macrophages begin to migrate to the wound, peaking by day 5. These cells ingest cellular debris and also aid in activation of fibroblasts and promote collagen formation. Simultaneously, the process of re-epithelialization is occurring. This process starts as early as 12 hours after the injury, and after 24-48 hours the re-epithelialized layer is impermeable to water. New capillaries, arterioles, and lymphatics form or repair during days 3-7 in a process known as neovascularization, which helps sustain the growing tissue by increasing blood flow to the wound bed. Fibroblasts, with support from macrophages, are already forming collagen, with the process accelerated by the proliferation of new blood vessels providing oxygen and nutrients to the wound bed, with peak synthesis of collagen between days 5-7. The wound then begins to contract during a process called remodeling, which continues for several months. This balance between growth and contraction creates a time period, usually around days 7-10, in which the wound is most prone to dehiscence.4
Each of these stages can be influenced by the medical professional during repair, and then by wound care post-repair. The process of epithelialization can be impeded by factors such as bacterial inoculation or infection and excessive wound debris, or enhanced by factors such as adequate moisture level and appropriate wound approximation. Neovascularization and resultant granulation tissue formation can be disturbed by vigorous washing or application of high concentration disinfectants. The timing of collagen formation and maximum wound tensile strength dictates when sutures should be removed, generally within 5-10 days depending on location, severity, vascularity, and wound tension. Wounds generally reach maximum tensile strength between 3 and 12 months.4,5
Cosmetic outcomes are naturally important to most patients, and all patients should be counseled on this aspect of wound healing.6 All wounds will contract and form scar tissue, but utilizing proper suture placement techniques can minimize these effects. Placing the suture with the needle held perpendicular to the skin surface will evert the skin and will result in a more cosmetically acceptable scar. Contrarily, if the needle is held at a shallow angle, it will cause tissue inversion and a depressed scar, which will be more noticeable and have decreased tensile strength.
Skin is an elastic membrane, and its appearance and functionality across the body relates to static and dynamic skin tension due to adherence to the underlying tissue, and to the activity of muscle and joint movements. This is clinically noticeable by the retraction of skin edges when a laceration occurs, exposing the underlying tissue.7 The width of retraction relates to the inherent skin tension in the area of the wound, and can dynamically change if the wound is in a location with significant flexion and extension stresses such as the elbow. Generally, the more marked the amount of retraction, the higher the risk for dehiscence and the wider the scar after repair. This can be addressed during wound repair using techniques to reduce overall tension, such as vertical or horizontal mattress sutures, multilayer repair, or temporary splinting. When discussing the issue of scar formation, it is also important to note whether or not the patient has a known tendency to form keloid scars, in which case the patient should be warned about this possible outcome and referred to a plastic surgeon for close follow up.7
Wound Infection
Wound infection causes delayed healing, decreased tissue scar strength, poor cosmetic outcomes, and, not surprisingly, decreased patient satisfaction. One of the primary goals of wound care is infection prevention. The overall incidence of wound infection varies depending on what study is cited, but is most often reported as 2-3%.6,8 Factors leading to increased risk of infection include advanced age, poor nutrition, obesity, immune compromised states, initial bacterial contamination and burden of wound, and diabetes mellitus.6 Increased time before wound closure, usually stated as greater than 8 to 12 hours, is often cited as a risk for infection; however, this is not fully supported by the evidence presented in several recent reviews of the subject.6-8
A bacterial count of greater than 105 bacteria per gram of tissue is an associated risk factor for infection. Contaminated wounds greater than 5 hours old tend to grow more than 105 bacteria per gram of tissue.7 Locations on the body with greater than 105 bacteria per gram of tissue include the mouth, vagina, perineum, axilla, hands, feet, and scalp. The high vascularity of the face and scalp help to reduce the risk of infection in these areas, but the relative low vascularity of the extremities leads to a higher rate of infection in these areas, particularly the hands and feet. Using epinephrine in these areas can lead to decreased blood flow and could potentially lead to higher rates of infection.4 Patients with wounds to the hands and the feet, particularly if they have an underlying immunocompromised state such as diabetes, should be counseled about the increased risk of infection and to be vigilant about wound surveillance.
Planning the Procedure
As with all procedures that could result in exposure to biologically active material, universal precautions should be followed for protection of both the clinician and patient.7 Soap and water or an alcohol-based scrub should be used to wash and decontaminate the hands. Either sterile or non-sterile gloves should be used; historically, sterile gloves have been the standard of care during laceration and wound repair. Recent evidence, however, has not shown any increase in the risk of infection when clean, nonsurgical exam gloves are worn during wound repair.9 Surgical gloves do have the advantage of better fit, allowing for greater dexterity, but are more expensive. A mask with face shield or goggles for eye protection should also be utilized throughout the procedure, particularly when using irrigation and when injecting anesthetic. Adequate lighting is a necessity for optimal visualization of the wound. The patient should be placed in as comfortable a position as possible for the duration of the evaluation, preparation, and repair. When possible, the clinician should sit down for the procedure, and ideally the patient should be lying down or in a reclined position.10
During initial evaluation, counsel the patient on what to expect during the procedure, and also discuss factors that could lead to delayed or poor wound healing. Diabetes; crush injuries; large, jagged, or nonlinear wounds; distal extremity wounds; and contaminated wounds are all associated with a higher incidence of wound infections, poor wound healing, and suboptimal cosmetic outcomes.6,11
The timing of wound closure should be considered during the initial evaluation of the wound. Time after injury, wound location, and mechanism of wound are important factors to consider when deciding to close a wound immediately (primary closure) or after a period of delay and reevaluation (delayed closure). Scalp and face wounds can generally be closed within 12-24 hours of injury,4,6 while closure of hand or extremity wounds should generally occur sooner, within 10 hours of injury.6,12 Delayed primary wound closure should be considered in wounds that are greater than 10 hours old, contaminated by large amounts of biological material or debris, or wounds that may evolve over time, such as crush injuries or animal bites. The initial management should be the same for any wound, with copious irrigation and debridement with removal of nonviable tissues. In the case of delayed repair, the bacterial count will generally decrease over 2-4 days, assuming initial appropriate irrigation and debridement, and further nonviable tissue and debris will further demarcate.7 After initial evaluation, the wound should be dressed in sterile saline gauze and reevaluated in 2-3 days for signs of infection, need for further debridement, and appropriateness of delayed repair.
Evaluation of the Traumatic Wound
The most immediate concern during the evaluation of a traumatic wound is active hemorrhage. The majority of wound hemorrhage can be controlled with direct pressure. If bleeding does not stop through direct pressure alone, absorbable collagen or fibrin sealant placed directly on the wound in the area of hemorrhage is often successful. Care should be used in any attempt to clamp a blood vessel, as this can cause significant damage to the vessel itself and may risk damage to other vital structures in the area, including nerves, tendons, and adjacent vascular structures.
In the setting of uncontrollable arterial extremity bleeding, a tourniquet above the joint proximal to the injury is often successful in stopping hemorrhage — allowing for full exploration of the wound in a dry field. A blood pressure cuff can be utilized in this setting, inflated until bleeding ceases, allowing for wound evaluation, and then slowly deflated to identify the specific source of hemorrhage. If exsanguination is not a risk, the cuff should be deflated after approximately 20 minutes to prevent vascular and nerve compromise of the limb. If the bleeding cannot be controlled, the tourniquet should remain in place and the wound should be explored further in the operative setting. A neurovascular exam of the injured extremity should be conducted prior to and after application of a tourniquet, and should be documented in the patient’s chart.
Once bleeding is controlled, wound exploration can commence. Explore the depth of all wounds. Occasionally, this will require wound extension to fully examine surrounding structures such as tendons and joints, and to evaluate for foreign bodies. Prior to using local or regional anesthesia, a focused neurological exam distal to the wound must be conducted to determine if there is any nerve injury. A motor examination is essential throughout the extremities, but a sensory exam including two-point discrimination is important for areas involved in fine motor skills, such as the hand and fingers. A vascular exam should also be documented specifically evaluating distal pulses, skin color, tactile temperature, and capillary refill. All joints and muscle groups should be isolated and evaluated for tendon, ligament, or joint injury.4,7 If there is concern for joint compromise, saline with or without methylene blue can be injected into the joint, and then observed for extravasation with movement.13 Unfortunately, this technique does not have the sensitivity to completely rule out joint involvement, and if there is a high suspicion for injury, immediate evaluation or follow-up with an orthopedist is recommended.
Preparation for Wound Repair
The wound must be thoroughly examined and explored prior to repair. The main objective of wound exploration is the removal of any substance, foreign body, or devitalized tissue that can facilitate infection or delay wound healing. Wound contaminants can be organic or inorganic in nature. Common contaminants include fresh water, wood, glass, metal, gravel, dirt, hydrocarbons, and saliva. Manual removal of larger foreign bodies should be accomplished as soon as possible, the wound should then be further debrided with moist gauze, and afterward copiously irrigated to remove finer particles and reduce bacterial burden. There have been several studies and literature reviews that indicate tap water is equivalent to sterile normal saline for wound irrigation in the emergency department.14-16 Volume appears to be the main variable for adequate irrigation, and tap water often provides the mechanism for highest irrigant volume. The volume of irrigation varies in practice. Available studies indicate amounts between 200-500 mL per wound, as well as wound surface area-based protocols where approximately 50 mL of fluid per cubic centimeter of wound is utilized are appropriate.7,14-16 Based on this clinical variation, 500 mL of fluid for an average wound is likely adequate; however, clinicians must use their own judgment when evaluating for adequate wound irrigation. Wounds that have high levels of debris contamination, high bioburden debris such as stool, or that occur in immunocompromised patients should be more aggressively irrigated. The amount of irrigant and time of irrigation should always be documented in the chart.
Plain film radiographs should be obtained of any wounds that have a high likelihood of retained foreign body, i.e., broken glass, road rash, or penetrating injuries. Metal fragments are easily seen on plain films. Plain films are generally able to detect glass if the size is greater than 1 mm, and can detect glass fragments larger than 2 mm with a sensitivity above 95%.17 The depth of glass fragments affects the detection rate, with a miss rate of 4% in superficial fragments, increasing to 11% for deeper fragments.18 Many foreign bodies are potentially undetectable by X-ray, notoriously wood, other vegetative materials, and plastic material. Ultrasound can detect wood fragments and other foreign bodies that are not usually seen by plain film. A high frequency linear probe should be used to evaluate the site of injury. The size of the object that can be detected by ultrasound will vary depending on the probe used, as changing the frequency will change the resolution, so the highest frequency probe available should be used to evaluate for foreign bodies. When viewed under B mode, foreign bodies will appear as bright objects, usually with distortion of any structures deep to the foreign body, an effect known as “dirty shadow.” Depending on the operator and the level of training, ultrasound has been shown to have a sensitivity between 40-72% in these cases.19 Although ultrasound does miss foreign bodies made from radiolucent materials, it is superior to X-ray for initial evaluation of radiolucent foreign bodies despite its limitations.20 If there is still concern for foreign bodies not seen on X-ray or ultrasound, a CT scan can be obtained.21
The possibility of retained foreign bodies and the signs and symptoms of infections should be discussed at length with the patient, and this conversation should be documented in the chart. The sensation of a foreign body by the patient is an indicator that there may be retained material in the wound that was missed during the initial exploration, particularly if the wound was caused by a glass fragment.22 Repeat radiographic evaluations are reasonable to assure foreign body removal.
Further decreasing the bacterial burden of the wound and surrounding tissue is accomplished with antiseptic solutions. Cleansing the area surrounding the wound with iodophor (10% betadine) solution is recommended. Betadine solution is preferred over betadine scrub because the scrub form contains detergent, which may damage exposed tissues. A dilute solution can be used (less than 1%) in the wound and along the wound margins, as higher concentrations are toxic to exposed epithelial cells and other exposed tissues.4,5 Hair can be adequately cleaned in the same manner as the skin, and usually does not need to be clipped. If hair must be moved out of the way, use petroleum jelly antibiotic ointment to reposition and hold the hair in place. If hair must be removed for better visualization or closure, use clippers and do not shave the hair. Shaving unnecessarily exposes the base of hair follicles and causes microscopic injury to the surrounding epithelium, providing a mechanism for bacterial invasion and increasing the rate of wound infection.5
Inspect the wound for any necrotic or nonvascularized tissue, heavily macerated tissue, or minimally adherent subcutaneous fat nodules. These should be removed, as these devitalized tissues will act as a nidus for bacterial growth and infection. Sharp scissors are the best instrument for this task.4,5
Pain Control and Types of Anesthesia
Perform anesthesia early in the course of evaluation. Pain is often undertreated by emergency medicine physicians,23 and there are many available options for pain management in traumatic wounds. The patient should be aware of possible options and included in the decision-making process.24 Options include local infiltration of the wound, topical anesthetics, regional anesthesia, conscious sedation, and, rarely, operative sedation. The most appropriate option depends on many factors, including hemodynamic stability, physical exam findings, age, allergies, wound size, and the patient’s previous experiences with anesthesia.
One percent lidocaine without epinephrine is the most commonly used local anesthetic injected into the wound site; however, bupivacaine is more often used for regional nerve blocks.25 Bupivacaine has a longer duration of action than lidocaine but is less frequently used in the ED setting, although it has a similar safety profile to that of lidocaine.25 The maximum dose of lidocaine is 4 mg/kg in a single injection of plain lidocaine, or 7 mg/kg if epinephrine is used.5,25 Considering that the standard 1% lidocaine for cutaneous anesthesia is 10 mg/mL, the maximum dose of lidocaine is much larger (approximately 30 mL) than is given in the routine setting of laceration repair. If there are multiple large lacerations or extremely long lacerations, though, this may be a concern. Epinephrine-containing local anesthetics decrease wound hemorrhage, prolong anesthesia, and permit higher doses of anesthetic, making it an ideal adjunct for wound repair. However, the routine use of epinephrine should be avoided in wounds that are highly contaminated, as it may impede blood flow to the area and increase the risk of infection and delay wound healing.7 In the emergency department setting, regional blocks are often utilized in the form of digital blocks, facial blocks, and penile blocks. More extensive blocks are generally done under the direction of an anesthesiologist. Classically, it has been taught that epinephrine should not be used in certain regional blocks, such as digital blocks and penile blocks, with concern for possible vasospasm and resultant distal tissue injury, but recent literature argues for the safety of epinephrine.29
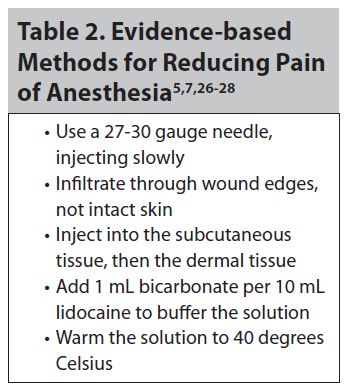
Occasionally, patients will report an allergy to local anesthetics. This is often an allergy to the preservative methylparaben, which is frequently used in shelf anesthetics, as opposed to the anesthetic itself. In these cases, cardiac lidocaine can be utilized. If a patient reports an allergy to one of the amide class of anesthetics, an ester class anesthetic, such as tetracaine, can be used with little if any risk for cross-reactivity.25 An alternative to the amide and ester anesthetics is local infiltration of 0.5-1% diphenhydramine and 1% saline; however, pain of injection is reportedly greater with these formulations, although it should be noted that this is an off-label use of diphenhydramine and saline and may not be appropriate depending on the clinical situation or institutional policies. Epinephrine, diphenhydramine, and saline injections should be avoided in areas with poor collateral circulation, as there may be a small risk of tissue necrosis.30-32 Evidence-based methods for reducing pain of anesthesia are shown in Table 2.
Topical anesthetics (see Table 3) are often used in the pediatric population, and are associated with less discomfort to the patient during application when compared to injectable anesthetics.33,34 LET (lidocaine 4%, epinephrine 0.1%, and tetracaine 0.5%) is available as both a solution and a gel. LET has been shown to be as effective in controlling pain as injected lidocaine, from both a patient and a physician perspective. LET can easily be applied by nursing staff, and has been shown to be effective and efficient when applied in triage.35,36 LET is most often used for lacerations to the face and scalp where the epidermis is relatively thin, but can be used on any external location. TAC (tetracaine 0.5%, adrenaline 1:2000, cocaine 11.8%), does not appear to be any more effective than LET.36 Fatal side effects of TAC have been reported in younger children when used on mucosal surfaces, but it seems to be safe when used in children older than 5 years old with appropriate dosing and close supervision.37
Table 3. Common Topical Anesthetics and Locations of Use
|
Topical |
Intact Skin |
Wound |
|
LET |
X |
|
|
TAC |
X |
|
|
EMLA |
X |
|
|
LMX |
X |
|
|
Skin refrigerant |
X |
EMLA (2.5% lidocaine and prilocaine) and LMX (4% lidocaine) are often applied to intact skin before venipuncture or abscess drainage; however, these mixtures take 45-120 minutes for maximal effectiveness and their benefit has been reported inconsistently in the literature.37 Sequential layered application of topical lidocaine and epinephrine was shown to be less painful than infiltrated lidocaine; however, a significantly longer time period for application was required.38
Consider conscious sedation for patients who have extensive injuries that may require large amounts of local anesthetics, for patients who are unlikely to tolerate the procedure, and for patients with inadequate pain control. For wound repair, sedation is most often utilized in the pediatric patient. Propofol and ketamine are two of the most common and well-studied medications used for sedation. When compared in adult patients, ketamine and propofol have a similar safety profile and are similarly effective in controlling patient discomfort during the procedure.39 Propofol is dosed at 1 mg/kg initially, followed by 0.5 mg/kg every 1-2 minutes until sedation is achieved. The major concerning side effects are respiratory depression and hypotension, but are generally rare and easily managed.
Ketamine is dosed intravenously at 1-2 mg/kg, and can also be given intramuscularly at 2–4 mg/kg. Ketamine offers some physiologic advantages including relative preservation of respiratory function and blood pressure when compared to other sedative medications, and provides additional analgesic properties. Laryngospasm is a rare but potentially serious adverse reaction with ketamine. An “emergence” phenomenon can also be encountered; as the sedative effects dissipate, the patient can emerge agitated and dysphoric. If an emergence reaction occurs, the treatment is low dose benzodiazepines, i.e., midazolam 1 mg IV.39,40 Alternatively, a benzodiazepine can be given prior to sedation and may help reduce the incidence of emergence reaction.41 There is some evidence to suggest that pretreatment with an antiemetic such as ondansetron can reduce the incidence of vomiting in children; however, this is not standard of care and there are only anecdotal reports of this practice in adults.42
A mixture of propofol and ketamine, referred to informally as “ketofol,” has also been studied, and has been shown to be effective, safe, and easy to use. The two medications are mixed together in a 1:1 ratio of 10 mg/mL of both ketamine and propofol, in a single syringe. This mixture is then infused and titrated by the physician in 0.5 mg/kg aliquots every 1 minute until the desired level of anesthesia is acheived.43 The goal of this combination is to obtain adequate analgesia and sedation, while minimizing the unwanted side effects of the individual medications, and decreasing the total dose of medications.43,44 This combination was compared with combined midazolam and fentanyl, and was found to be equally effective with no increase in adverse effects.44
Suture Materials, Selection, and Applications
The choice of wound closure material should be based on provider experience, wound characteristics, patient preference, and availability. Ask the patient if he or she has an opinion based on previous experience, or what his or her perceived outcomes are from a particular closure material. Discuss these preferences early with the patient in order to help guide expectations for wound healing, follow up, and timing of suture or staple removal.
The primary materials used for wound closure are sutures, staples, and skin adhesives.
Sutures are the most common method of wound closure.4,5,11,45 The initial decision when selecting a suture material is whether to use absorbable (see Table 4) or non-absorbable sutures (see Table 5). Several studies have examined the cosmetic outcomes, scar formation, and patient satisfaction with the use of absorbable and non-absorbable suture. A meta-analysis did not appear to reveal any statistical difference between any of these outcomes; however, there have been no large, randomized controlled studies across age groups evaluating these two options.46 Absorbable sutures should be used in areas that are likely to heal over and make removal difficult, such as mucosal surfaces in the mouth or vagina. Absorbable sutures should be used for all deep sutures and whenever the wound must be closed in multiple layers. Absorbable sutures are also appropriate for patients with poor follow-up who are unlikely to return for suture removal, and for patients for whom removal will be difficult secondary to young age or agitation. Non-absorbable sutures should be used in areas that are at risk for poor wound healing, wounds under significant tension, and wounds over flexor and extensor surfaces.4,5,11,45,46
Table 4. Types of Absorbable Sutures
|
Brand Name/Suture |
Material |
Duration of |
Absorption |
|
Plain gut |
Sheep intestine mucosa |
5-10 days |
Variable |
|
Chromic gut |
Chromium trioxide |
10-21 days |
Up to 90 days |
|
Vicryl |
Polyglactin |
20-30 days |
30-120 days |
|
Dexon |
Polyglycolic acid |
20-30 days |
30-120 days |
|
Maxon |
Monofilament |
45 days |
180-200+ days |
|
PDS |
Monofilament |
45 days |
180-200+ days |
|
Caprosyn |
Monofilament |
14 days |
56 days |
|
Biosyn |
Monofilament |
21 days |
90-110 days |
Table 5. Types of Non-absorbable Sutures
|
Brand Name/Suture |
Material |
Tensile Strength |
|
Dermalon |
Nylon |
Intermediate |
|
Ethilon |
||
|
Prolene |
Polypropylene |
Greatest |
|
Surgilene |
||
|
Silk |
Silk |
Least |
Sutures come in either monofilament or braided forms. Monofilaments are less immune reactive, are associated with lower risk of infection, and result in less scarring when compared with braided suture materials. Most physicians choose monofilament material for these reasons.47 However, it should be noted that braided sutures generally have a higher tensile strength, and are at lower risk of spontaneous rupture.45
Staples are quicker and easier to place than sutures; however, they are slightly more complex to remove, with the resultant possibility of more pain. Skin staples are less biologically reactive and associated with less infection risk than sutures, and are especially good for lacerations in hair-covered areas, and long or straight lacerations involving the extremities or trunk. They have comparable cosmetic outcomes to sutures.48
Topical skin adhesives are liquid monomers that polymerize once exposed to moisture from the wound and the atmosphere. They form a hard, water-resistant, bonding substance over the wound. The adhesive remains on the skin and eventually sloughs off, usually in 7 to 10 days. There are several commercial preparations, nearly all based on the cyanoacrylate monomer. The octyl-cyanoacrylate monomer has been shown to have a higher tensile strength than butyl-cyanoacrylate, both of which have superior strength to surgical skin tapes.49,50 Skin adhesives are best utilized for linear wounds that are under little tension, and are often the method and material of choice for facial wounds and wounds in children. The advantage of using skin adhesives in children is twofold: 1) the application is much less uncomfortable and well tolerated; and 2) the child does not need to go through a second procedure for suture or staple removal.45,50
Skin adhesives are applied by approximating the wound with either a gloved hand or sterile skin forceps, and then applying a small bead of glue linearly along the approximated wound. The skin should be held in close approximation for about a minute until the skin adhesive no longer feels tacky, at which point it is set and does not need any further dressing. Patients should be instructed that although the skin adhesive is waterproof, they should not soak the area, as this can lead to early sloughing of the adhesive.
Surgical skin tapes are an option for the same wound types as mentioned for tissue adhesives. Skin tapes have similar outcomes and similar infection rates as topical skin adhesives, but are associated with fewer complications.51 Skin tape and skin adhesives can be used in conjunction with good results, and have less dehiscence than when using skin adhesives alone. Skin tape should be applied first and then both the wound and the tape coated with tissue adhesive.45,52 Skin tape can also be used in flap wounds where the tissue is too thin for sutures.21
Post Procedure Care
The timing of suture, staple, or tape removal is dependent upon the location and the material used. Table 6 gives a general guideline for how long sutures or staples should remain in place.4,5
Table 6. Timing of Suture Removal
|
Location |
When to Remove |
|
Face |
3-5 |
|
Scalp |
7 |
|
Trunk |
7-10 |
|
Extremities |
10-14 |
|
Fingertip |
10-12 |
|
Palms/soles |
14 |
|
Extensor joints |
14 |
|
Joints |
8-10 |
Facial sutures are removed more quickly in order to prevent “railroad tracks” from forming. This is a crosshatched scar resulting from epithelialization and keratinization of the suture puncture marks perpendicular to the wound bed. These generally occur when sutures are left in place greater than 8 days after wound repair.45 After removing sutures from the face, apply skin tape to decrease the likelihood of dehiscence, as wound tensile strength is extremely low this early in healing.
Prophylactic antibiotics have not been well supported in the civilian medical literature or textbooks.5,53-55 A military study showed that in penetrating injuries, antibiotics reduced infection rates from 23.1% to 4.2% and irrigation decreased infection rates from 44% to 2%.56 If a wound is contaminated and has the potential for infection, antibiotics are indicated, and should be administered as soon as possible to achieve adequate blood and tissue levels. (See Table 7.)54.55
Table 7. Indications for Prophylactic Antibiotics54,55
|
Consensus Indications |
|
|
Relative indications (base on clinical judgment) |
|
Historically, the first-line antibiotic for prophylaxis has been a first-generation cephalosporin, such as cephalexin. The recent increase in MRSA infections and isolates argues for the use of antibiotics that appropriately cover this pathogen, such as clindamycin or a combination of cephalexin and trimethoprim sulfamethoxazole. Amoxicillin-clavulanate or clindamycin should be considered if contamination by anaerobes is suspected, as in wounds contaminated by feces.11 Tetanus prophylaxis is based on the state of the wound, and if the patient has previously received the full three-dose primary vaccination series. (See Table 8.)
Table 8. Tetanus Vaccines and TIG for Wound Management
|
Age (years) |
Vaccination history |
Clean, minor wounds |
All other wounds |
|
* Pregnant Women: As part of standard wound management care to prevent tetanus, a tetanus toxoid–containing vaccine might be recommended for wound management in a pregnant woman if 5 years or more have elapsed since the previous Td booster. If a Td booster is recommended for a pregnant woman, health-care providers should administer Tdap. Source: Centers for Disease Control and Prevention, Emergency Preparedness and Response, Tetanus Prevention After a Disaster, http://www.bt.cdc.gov/disasters/disease/tetanus.asp. |
|||
|
0 through 6 |
Unknown or not up-to-date on DTaP series based on age |
DTaP |
DTaP TIG |
|
Up-to-date on DTaP series based on age |
No indication |
No indication |
|
|
7 through 10 |
Unknown or incomplete DTaP series |
Tdap and recommend catch-up vaccination |
Tdap and recommend catch-up vaccination TIG |
|
Completed DTaP series AND < 5 years since last dose |
No indication |
No indication |
|
|
Completed DTaP series AND ≥ 5 years since last dose |
No indication |
Td, but Tdap preferred if child is 10 years of age |
|
|
11 years and older (*if pregnant, see footnote) |
Unknown or < 3 doses of tetanus toxoid-containing vaccine |
Tdap and recommend catch-up vaccination |
Tdap and recommend catch-up vaccination TIG |
|
3 or more doses of tetanus toxoid-containing vaccine AND < 5 years since last dose |
No indication |
No indication |
|
|
3 or more doses of tetanus toxoid-containing vaccine AND 5-10 years since last dose |
No indication |
Tdap preferred (if not yet received) or Td |
|
|
3 or more doses of tetanus toxoid-containing vaccine AND > 10 years since last dose |
Tdap preferred (if not yet received) or Td |
Tdap preferred (if not yet received) or Td |
|
Repairing Special Locations
Scalp wounds are best evaluated after trimming hair, either with scissors or clippers. A series of figure of eight suture or skin clips should be used to control hemorrhage that does not stop with direct pressure alone. Once hemostasis is achieved, the wound should be evaluated for galeal injury. Any defect in the galea should be closed with absorbable suture before placing any superficial sutures. This improves cosmesis and lowers the risk of catastrophic infection. The scalp is an ideal location for skin staples, as long as the galea is intact or after closing the galea with appropriate sutures. These wounds rarely become infected as there is excellent blood flow, and unless the wounds are grossly contaminated or contain numerous foreign bodies, they rarely need prophylactic antibiotics. Patients should be instructed to wait 24-48 hours before washing their hair.
Facial wounds, including those on the eyelid, nose, lip, and ear, may require a specialist if complicated, but are generally within the scope of practice of emergency practitioners. Absorbable sutures should be used for deep layers whenever possible, as this will relieve superficial tension, appropriately align the dermis, and allow for a more cosmetic closure. Utilize 6-0 suture for superficial closure and take care to ensure appropriate wound eversion. As wounds heal, the edges will become slightly depressed, and if the wound is closed without appropriate eversion, the resultant scar may be depressed and thus more noticeable.
Lip lacerations are often best anesthetized via infraorbital and submental nerve blocks. These blocks allow for adequate analgesia without distortion of the wound margins, allowing for more anatomically correct alignment and better cosmetic results. The initial and most critical portion of lip laceration repair involves precise approximation of the vermillion border, as even small discrepancies can become very noticeable after healing. If the laceration is through the entire lip, close the intraoral portion first with absorbable suture and the external portion last, using deep sutures if necessary for a multilayered approach.
Lacerations involving the nose require intranasal exploration, with the nasal septum specifically inspected for lacerations and septal hematomas that would require drainage. If the nostril is involved, it must be reapproximated carefully, often via layered approach, to avoid asymmetry. Any lacerations over exposed cartilage should be irrigated and closed as soon as possible. If there is a nasal bone fracture underlying a laceration, this should be treated as an open fracture with appropriate antibiotics.
Lacerations involving the eyelid must be inspected thoroughly, with careful evaluation of the surrounding structures including the lacrimal duct, tarsal plate, and globe. Referral to an ophthalmologist, either urgently or emergently depending on degree of injury, should occur for any laceration involving the lid margin, the medial third of the lower lid, or for suspicion of open globe. Visual acuity should be documented, and the eye should be evaluated for hyphema, iritis, and corneal abrasion. Do not shave the eyebrow, as 20% will either not grow back or will grow back irregularly. A supraorbital nerve block provides adequate anesthesia and will prevent distortion of wound edges for forehead and eyebrow lacerations. Colored nylon suture can be used for lacerations through the eyebrow, as this will help distinguish the suture from eyebrow hair during repair and during suture removal.
Ear lacerations are closed first anteriorly and then posteriorly. If the cartilage needs to be repaired, an absorbable suture with a longer duration of tensile strength should be utilized. If a perichondral hematoma is present either before or after repair, it must be drained to avoid the potential for permanent deformation. Once the ear is repaired, a compression bandage should be applied for at least 24 hours to prevent further fluid collection and to help maintain the shape of the ear.
Hand wounds require careful evaluation and often exploration. The patient should perform a full range of motion, with close evaluation of full extensor and flexor movements. The wound should also be explored in the position of injury, as tendon, joint, vascular, and nerve injuries are common and the superficial appearance of the laceration can cause an underestimation of the wound depth and of injury to the underlying structures. A laceration may need to be extended if a thorough exam is impossible secondary to the small size of the wound. Any laceration to the hand that occurs during an altercation should be considered the result of a dental penetrating injury, or “fight bite,” and should be prophylactically treated with amoxicillin-clavulanate, as these are at great risk for aggressive infection. Consider either immediate consultation or urgent follow up with a hand surgeon for complicated wounds, such as those with injury to the tendon, nerve, or vasculature.
Digital blocks allow for adequate pain control and do not distort distal tissues, allowing for easier exploration and better alignment of wound edges. Lacerations of the fingertip that include the nail bed can be repaired with 6-0 absorbable suture after removal of the nail, and then either a clean semi-rigid material or the nail itself can be placed in the potential space between the nail bed and cuticle. This helps to preserve the germinal matrix and to prevent adhesion and resultant nail deformities as the nail regrows. Subungual hematomas do not require nail removal to inspect for nail bed laceration. These can be safely trephinated with a cautery device or an 18-gauge needle, which allows for self-evacuation of the hematoma and nearly immediate pain relief for the patient.57,58
Recent research has shown that the pretibial area is an area at risk for poor healing, and that for every 1 cm increase in wound size, there is a 30% reduction in the healing rate.59 This should be discussed with the patient to help set expectations. These wounds, if not gaping, can be closed with steri-strips with no change in outcomes.60
Puncture wounds of the foot often require X-rays to evaluate for foreign bodies. Routine tissue coring and high-pressure irrigation is not recommended; simple exploration and irrigation usually suffices for adequate treatment. Prophylactic antibiotics are not well studied for puncture wounds to the foot, but consider ciprofloxacin for deep puncture wounds over the forefoot or through the sole of a shoe. Regional nerve blocks of the foot may be better tolerated than trying to inject into the thick plantar skin or around calluses.21
Tips/Tricks
In summary, approach the patient with a traumatic wound in the following manner:
- Obtain a detailed history of the trauma and assess for risk factors associated with poor wound healing.
- Optimize the procedure by placing the patient supine and ensure adequate lighting and exposure.
- Determine and continually reassess the most appropriate method of anesthesia.
- Thoroughly explore, irrigate, and debride the wound.
- Use skin adhesives with or without tape for superficial wounds under light tension.
- Use absorbable sutures for mucosal surfaces and deep sutures, and consider their use in children. Use non-absorbable sutures for wounds subject to movement or under high tension.
- Educate the patient on proper aftercare, and on the unavoidable nature of scar formation.
- Do not routinely give prophylactic antibiotics to the healthy patient with a simple non-contaminated wound, and ensure tetanus immunization is complete.
References
- Singer AJ, Thode HC Jr, Hollander JE. National trends in ED lacerations between 1992 and 2002. Am J Emerg Med 2006;24(2):183-188.
- Karcz A, Korn R, Burke MC, et al. Malpractice claims against emergency physicians in Massachusetts: 1975-1999. Am J Emerg Med 1996;14(4):341-345.
- Henry GL, Sullivan DJ. Emergency Medicine Risk Management: A Comprehensive Review, 2nd edition. Dallas: American College of Emergency Physicians;1997.
- Trott AT. Surface Injury and Wound Healing. In: Wounds and Lacerations: Emergency Care and Closure. Third Edition. Philadelphia: Mosby Inc; 2005: 22-25.
- Nicks BA, Ayelio EA, Woo K, et al. Acute wound management: Revisiting the approach to assessment, irrigation, and closure considerations. Int J Emerg Med 2010;3(4):399-407.
- Quinn JV, Polevoi SK, Kohn MA. Traumatic lacerations: What are the risks for infection and has the ‘golden period’ of laceration care disappeared? Emerg Med J Published Online First: January 12, 2013 as 10.1136/emermed-2012-202143, accessed on April 28, 2013.
- Edlich RF, Rodeheaver GT, Thacker JG, et al. Revolutionary advances in the management of traumatic wounds in the emergency department during the last 40 years: Part I. J Emerg Med 2010;38(1):40–50.
- Zehtabchi S, Tan A, Yadav K, et al. The impact of wound age on the infection rate of simple lacerations repaired in the emergency department. Injury 2012;43:1793–1798.
- Perelman VS, Francis GJ, Rutledge T, et al. Sterile versus nonsterile gloves for repair of uncomplicated lacerations in the emergency department: A randomized controlled trial. Ann Emerg Med 2004;43(3):362-370.
- Johnson RL, Sadosty AT, Weaver AL, et al. To sit or not to sit? Ann Emerg Med 2008;51:188-193.
- Singer AJ, Hollander JE. Methods for wound closure and postrepair wound care. In: Tintinalli, JE, et al, eds. Tintinalli’s Emergency Medicine - A comprehensive study guide, 7th edition. Chicago: McGraw Hill Medical; Chicago: 356-360.
- Patel R, Lakdawala VS, Prasankumar R, et al. Abstract #240: Is there an optimal time from injury for laceration primary wound closure to minimize wound infection rates? Acad Emerg Med 2010;17(5):S83. Abstract only.
- Konda SR, Howard D, Davidovitch RI, et al. The saline load test of the knee redefined: A test to detect traumatic arthrotomies and rule-out periarticular wounds not requiring surgical intervention. J Orthop Trauma 2013;27(9):491-497.
- Weiss EA, Oldham G, Lin M, et al. Water is a safe and effective alternative to sterile normal saline for wound irrigation prior to suturing: A prospective, double-blind, randomised, controlled clinical trial. BMJ Open. 2013;3(1):1-6.
- Cooper DD, Seupaul RA. Is water effective for wound cleansing? Ann Emer Med 2012;60(5):626-627.
- Moscati RM, Mayrose J, Reardon RF, et al. A multicenter comparison of tap water versus sterile saline for wound irrigation. Acad Emerg Med 2007;14(5):404-409.
- Chisolm CD, Wood CO, Chua G, et al. Radiographic detection of gravel in soft tissue. Ann Emerg Med 1997;29:725-730.
- Weinberger LN, Chen EH, Mills AM. Is screening radiography necessary to detect retained foreign bodies in adequately explored superficial glass-caused wounds? Ann Emerg Med 2008;51(5):666-667.
-
Crystal CS, Masneri DA, Hellums JS, et al. Bedside ultrasound for the detection of soft tissue foreign bodies: A cadaveric study.
J Emerg Med 2009;36(4):377-380. Epub 2008 Oct 18. - Manthey DE, Storrow AB, Milbourn JM, Wagner BJ. Ultrasound versus radiography in the detection of soft-tissue foreign bodies. Ann Emerg Med 1996;28(1):7-9.
- Singer AJ, Dagum AB. Current Concepts: Current management of acute cutaneous wounds. N Engl J Med 2009;359:1037-1046.
- Steele MT, Tran LV, Watson WA, et al. Retained glass foreign bodies in wounds: Predictive value of wound characteristics, patient perception, and wound exploration. Am J Emerg Med 1998;16(7):627-630.
- Bhargave R, Young KD. Procedural pain management patterns in academic pediatric emergency departments. Acad Emerg Med 2007;14:479-482.
- Flynn D, Knoedler MA, Hess EP, et al. Engaging patients in health care decisions in the emergency department through shared decision-making: A systematic review. Acad Emerg Med 2012;19(8):959-967.
- Dillon DC and Gibbs MA. Local and Regional Anesthesia. In: Tintinalli, JE, et al, eds. Emergency Medicine - A comprehensive study guide. 7th Edition. Chicago: McGraw Hill Medical:270-283.
- Bartfield, JM, Sokaris SJ, Raccio-Robak N. Local anesthesia for lacerations: Pain of infiltration inside vs outide the wound. Acad Emerg Med 1998;5:100-104.
- Hogan M, vanderVaart S, Perampaladas K, et al. Systematic review and meta-analysis of the effect of warming local anesthetics on injection pain. Ann Emerg Med 2011;58:86-98.
- Cattamanchi S, Papa MK, Trichur RV. Abstract #408: Randomized double-blind placebo-controlled trial comparing room temperature and heated lidocaine for local anesthesia and digital nerve block. Ann Emerg Med 2009;54:S129. Abstract only.
- Chowdhry S, Seidenstricker L, Cooney DS, et al. Do not use epinephrine in digital blocks: Myth or truth? Part II. A retrospective review of 1111 cases. Plast Reconstr Surg 2010;126(6):2031-2034.
- Green SM, Rothrock SG, Gorchynski J. Validation of diphenhydramine as a dermal local anesthetic. Ann Emerg Med 1994;23:1284-1289.
- Dire DJ, Hogan DE. Double-blinded comparison of diphenhydramine versus lidocaine as a local anesthetic. Ann Emerg Med 1993;22:1419-1422.
- Green SM. What is the role of diphenhydramine in local anesthesia? Acad Emerg Med 1996;3:198-200.
- Bhargave R, Young KD. Procedural pain management patterns in academic pediatric emergency departments. Acad Emerg Med 2007;14:479-482.
-
Grabinsky A, Sharar SR. Regional anesthesia for acute traumatic injuries in the emergency room. Expert Rev Neurother 2009;9(11):
1677-1690. - Ernst AA, Marvez-Valls E, Nick TG, et al. Topical lidocaine adrenaline tetracaine (LAT gel) versus injectable buffered lidocaine for local anesthesia in laceration repair. West J Med 1997;167(2):79-81.
- Ernst AA, Marvez-Valls E, Nick TG, et al. LAT (lidocaine-adrenaline-tetracaine) Versus TAC (tetracaine-adrenaline-cocaine) for topical anesthesia in face and scalp lacerations. Am J Emerg Med 1995;13(2):151-154.
- Bonadio WA. Safe and effective method for application of tetracaine, adrenaline, and cocaine to oral lacerations. Ann Emerg Med 1996;27:396-398.
- Gaufberg SV, Walta MJ, Workman TP. Expanding the use of topical anesthesia in wound management: Sequential layered application of topical lidocaine with epinephrine. Am J Emerg Med 2007;25:379-384.
- Miner JR, Gray RO, Bahr J, et al. Randomized clinical trial of propofol versus ketamine for procedural sedation in the emergency department. Acad Emerg Med 2010;17:604-611.
- Miner JR. Procedural Sedation and Analgesia. In: Tintinalli JE, et al, eds. Emergency Medicine - A comprehensive study guide, 7th edition. Chicago: McGraw Hill Medical;283-291.
- Sener S, Eken C, Schultz CH, et al. Ketamine with and without midazolam for emergency department sedation in adults:randomized controlled trial. Ann Emerg Med 2011;57:109-114.
- Langston WT, Wathen JE, Roback MG, et al. Effect of ondansetron on the incidence of vomiting associated with ketamine sedation in children: A double-blind, randomized, placebo-controlled trial. Ann Emerg Med 2008;52:30-34.
-
Andolfatto G, Willman E. A prospective case series of pediatric procedural sedation and analgesia in the emergency department using single-syringe ketamine–propofol combination (ketofol). Acad Emerg Med 2010;17:
194-201. - Nejati A, Moharari RS, Ashraf H, et al. Ketamine/propofol versus midazolam⁄fentanyl for procedural sedation and analgesia in the emergency department: A randomized, prospective, double-blind trial. Acad Emerg Med 2011;18(8):800-806.
-
Edlich, RF, Rodeheaver GT, Thacker JG, et al. Revolutionary advances in the management of traumatic wounds in the emergency department during the last 40 years: Part II.
J Emerg Med 2010;38(2):201-207. - Al-Abdullah T, Plint A, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: A meta-analysis. Pediatr Emerg Care 2007;23(5):339-344.
- Katz S, Izhar M, Mirelman D. Bacterial adherence to surgical sutures. A possible factor in suture induced infection. Surg 1981;194(1):35-41.
- Orlinsky M, Goldberg RM, Chan L, et al. Cost analysis of stapling versus suturing for skin closure. Am J Emerg Med 1995;13:77-81.
- Taira BR, Singer AJ, Rooney J, et al. An in-vivo study of the wound-bursting strengths of octyl-cyanoacrylate, butyl-cyanoacrylate, and surgical tape in rats. J Emerg Med 2010;38(4):546-551.
- Farion K, Osmond MH, Hartling L, et al. Tissue adhesives for traumatic lacerations in children and adults. Cochrane Database Syst Rev 2002;3:CD003326.
- Zempsky WT, Parrotti D, Grem C, et al. Randomized controlled comparison of cosmetic outcomes of simple facial lacerations closed with Steri Strip Skin Closures or Dermabond tissue adhesive. Ped Emerg Care 2004;20:519-524.
- Singer AJ, Chale S, Giordano P. Abstract #36: Evaluation of a novel wound closure device: A randomized clinical trial. Acad Emerg Med 2011;18:S15-S16. Abstract only.
- Zehtabtchi S. The role of antibiotic prophylaxis for prevention of infection in patients with simple hand lacerations. Ann Emerg Med 2007;49:682-689.
- Moran GJ, Talan DA, Abrahamian FM. Antimicrobial prophylaxis for wounds and procedures in the emergency department. Infect Dis Clin N Am 2008;22:117–143.
- Ong S, Moran GJ, Krishnadasan A, et al. Antibiotic prescribing practices of emergency physicians and patient expectations for uncomplicated lacerations. West J Emerg Med 2011;12(4):375-380.
- Gerhardt RT, Matthews JM, Sullivan SG. Abstract #212: The effect of systemic antibiotic prophylaxis and wound irrigation on penetrating combat wounds in a “return-to-duty” population. Ann Emerg Med 2008;52:S108. Abstract only.
- Seaberg DC, Angelos WJ, Paris PM. Treatment of subungual hematomas with nail trephination: A prospective study. Am J Emerg Med 1991;9(3):209-210.
- Roser SE, Gellman H. Comparison of nail bed repair versus nail trephination for subungual hematomas in children. J Hand Surg Am 1999;24(6):1166-1170.
-
McClelland HM, Stephenson J, Ousey KJ, et al. Wound healing in pre-tibial injuries — an observation study. Int Wound J 2012;9(3):
303-310. - Lo S, Hallam MJ, Smith S, et al. The tertiary management of pretibial lacerations. J Plast Reconstr Aesthet Surg 2012;65(9):1143-1150.
Traumatic wounds are a common cause of ED visits and are often managed exclusively by the emergency medicine provider. Most of these patients are evaluated, appropriately treated, and discharged with satisfactory outcomes. Although outcomes are similar, there are no specific preferred treatments for traumatic wound injuries, and this requires the emergency provider to develop comprehensive efficacy strategies on how to approach these common injuries. Wound closure materials, techniques, and management strategies vary widely, with both the preferences of the physician and the patient influencing the final decisions.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.