Ocular emergencies: Don’t lose sight of the diagnosis
By J. Tucker Montgomery, MD, JD, FCLM, Attorney, Montgomery & Pierce, PLC, Knoxville, TN; and John L. Montgomery Jr., MD, FACS, Associate Clinical Professor of Ophthalmology, University of Tennessee College of Medicine, Knoxville, TN.
Editor’s note: The emergency physician (EP) and nurse often may encounter patients with the chief complaint of eye pain or visual problems. Generally, the diagnosis easily is obtained and quickly treated. Unfortunately, a subset of patients will present with an illness that threatens permanent vision loss or impairment. EPs must have a broad differential diagnosis and structured approach in evaluating these patients to ensure appropriate diagnosis and treatment. Incorrect diagnosis by an EP of a patient with an ocular emergency that results in loss of vision can lead to a significant medical malpractice claim. Legal exposure can be reduced by adhering to a thorough and logical evaluation, good documentation, and when necessary, immediate consultation or referral. The purpose of this article is to guide the emergency practitioner in the evaluation of the patient with an ocular emergency. Following the recommendations detailed in this issue will help EPs and emergency department nurses develop risk management strategies and reduce the potential for ensuing malpractice litigation.
The Ocular History
Optimizing ocular care in the ED involves a logical evaluation of the patient complaint. Whether to treat and release or seek consultation with an ophthalmologist is dependent upon the EP’s ability to obtain and transmit useful and reliable information so an appropriate treatment plan can be formulated. The evaluation should begin with a thorough and thoughtful history starting with the chief complaint. Questions involving the present illness basically should answer "who, what, when, and where." The history of the present illness should include the symptoms, time of onset, the perspective of acute or chronic, and any precipitating event. A good outline of ocular history should be followed.1-5 See Table 1 for information to seek from an ocular history.
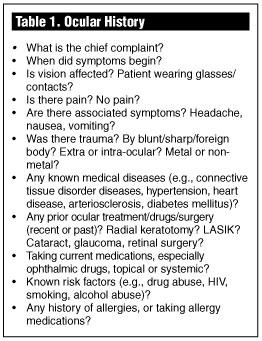
Emergency practitioners often consider the eye to be an organ that is independent of the body, and omit a careful review of systems to determine whether there are other systemic disease processes that could affect significantly the emergency problem/presentation. 6 For example, a history of diabetes mellitus, autoimmune disease, hypertension, heart disease, arteriosclerosis, or previous surgery should be taken. In patients who present with sudden unilateral loss of vision, history of long-standing type I diabetes, and a diminished or absent red reflex by ophthalmoscopic exam, the diagnosis of spontaneous vitreous hemorrhage would be high on the differential diagnosis list.7
The Ocular Physical
Every ocular physical examination should begin with a check of visual acuity (commonly referred to as the vital sign of the eye). The patient’s correction (if available) should be taken with each eye separately, using a Snellen eye chart at 20 feet or at another distance as noted. If a chart is not available or is inconvenient because of other associated injuries or disabilities, the clinician can use a near reading card or ask the patient to read normal-sized newsprint at reading distance (18-20 ins.). It is important to emphasize that normal visual acuity may be present in the face of significant visual complaints (e.g., blurred or "spotty" vision). The complaint of a "change in vision" cannot always be documented as a measurable loss. For example, some patients with blurred vision still can see 20/20 on the Snellen chart. They may have significant off-axis corneal pathology, (e.g., peripheral corneal ulcer), vitreous pathology (e.g., inferior vitreous hemorrhage), or retinal detachment (with the macula spared). Therefore, do not disregard a patient’s visual complaint when a normal visual acuity is documented.
When performing the physical examination, one must keep in mind that the eyes usually are symmetrical (although asymmetry does not always equate to abnormality). The examiner should compare one eye to the other throughout the exam using the unaffected eye as the standard. If there is any asymmetry present, one must be suspicious of abnormality. An EP should have a routine that includes comparing the lids, checking for orbital and adnexal asymmetry, and evaluating the extraocular muscle movement in the six cardinal directions of gaze. The pupils are generally equal. However, about 15-20% of patients have a slight inequality (anisocoria). Nevertheless, normal, slightly asymmetrical pupils usually will react briskly to direct and consensual stimulation by light.
The anterior chamber depth can be evaluated by the use of a bright light and some type of magnification with a loupe. EPs may use the lens wheel with a "high plus" on the ophthalmoscope. One may assess the depth of the anterior chamber by bringing a light from the temporal aspect horizontal to the iris plane and look for an iris shadow nasally, indicating that the iris is bowing forward and the anterior chamber is shallow. This is especially important with the evaluation of a red eye for acute angle closure ("narrow angle") glaucoma. The possibility of a traumatically ruptured globe is suggested by a deeper than normal anterior chamber.
The ophthalmoscope also can be used for evaluating the external eye under magnification, using the higher power "plus" lenses on the wheel to evaluate asymmetry, irregularity, haziness, cloudiness of the cornea, and the presence of conjunctival or circumciliary injection (redness more concentrated at the limbus, i.e., the junction of the cornea and the sclera, an indication of anterior segment inflammation). A good ophthalmoscopic examination begins approximately 1.5-2 feet from the patient with the patient’s focus on some object directly behind the examiner. The examiner then can evaluate the red reflex — the reddish-orange light reflected back through the patient’s media (the cornea, lens, and vitreous). The clinician should compare the eyes and look for irregularities and differences in the red reflex. A diminished or absent red reflex indicates possible disease or injury of the eye and may prevent a successful ophthalmoscopic exam.
If a normal red reflex is found, the examiner then should move closer to the eye and, using the lens wheel, focus through the media (cornea, lens, and vitreous) to locate the optic nerve head. The optic nerve head confirms the position and is a landmark from which to begin the retinal examination, visualize and assess the cup/disc ratios, and check for any asymmetry. This also is a good screening for glaucoma; i.e., with enlarged discs (> 0.5 disc diameter) or asymmetry (> 0.2 disc diameter), the clinician should consider the patient a "glaucoma suspect." The vessels in each of the four quadrants can be evaluated for the presence of hemorrhage, exudates, and other pathological vascular or retinal changes.1-5
With any presentation involving a red eye, possible trauma, or foreign body, one may place a drop of fluorescein on the cornea, flush excess from the surface, and examine with a cobalt blue light for corneal staining indicative of corneal pathology. Any corneal fluorescein staining indicates some possible pathologic corneal abrasion, laceration, foreign body, etc. This test particularly is important to rule out dendritic keratitis due to herpes simplex of the cornea.7
Adjunctive equipment, such as a slit lamp or tonometer, may be an option for a clinician trained and experienced in their use. The use of confrontation fields may be helpful occasionally. A useful method is to ask the patient to count the examiner’s fingers with one eye occluded in each of the quadrants while he or she is holding fixation on the examiner’s eye. It is debatable as to whether dilating the pupil for fundoscopic exam is necessary. Dilation of the pupil carries the potential risk of precipitating angle closure glaucoma and may not add a great deal of information. In most cases, the ophthalmoscopic evaluation of the retina with dilated pupil may carry more risk than benefit in an ED setting. Certainly, as noted previously, an assessment of the red reflex and an undilated exam should be performed if indicated. See Table 2 for evaluations to consider when conducting an ocular exam.
Medical and Traumatic Presentation
The disease or traumatic processes listed in Table 3 represent a number of important diagnostic conditions. The list is not comprehensive, but indicates broad categories of pathologies described in standard texts and articles.8-12
The emergency practitioner must be cautious in the use of topical ophthalmic medication. As a general rule, ophthalmic steroids should not be used in ED patients due to the risk of exacerbating herpes simplex. No one should be prescribed or given "take home" topical anesthetics, nor should an eye be dilated with atropine. It is very important to understand and recognize the cardiovascular/autonomic effects of topical and systemic ophthalmic drugs, such as Diamox (systemic) and Timoptic (topical).13
The majority of ocular emergencies do not require immediate ophthalmologic consultation. For example, the nonpainful red eye due to subconjuctival hemorrhage or bacterial, viral, or allergic conjunctivitis can be treated and referred.14 Mild, blunt, or sharp "superficial" trauma causing corneal abrasion may be seen in follow-up evaluation. Patches may benefit some patients; however, emergency practitioners do not use them frequently. Some literature suggests caution with patch use, particularly if abrasion pathology is due to contact lens mechanism.15,16 A metallic, superficially imbedded, or surface foreign body of the cornea usually can be removed safely, patched, and referred. Using small, sharp needles for corneal foreign body removal may be dangerous; corneal "spuds" are a safer alternative. Attempts to aggressively remove rust rings in the ED are not indicated. Referral to the ophthalmologist for removal is safer. (Editor’s note: ED removal of rust rings should be performed only if the physician has a strong background and training in the procedure. While many EPs may feel comfortable performing the procedure, others may opt for referral. Regardless of the decision, referral to and follow up by an ophthalmologist is required.)
An ultraviolet burn or welder’s flash burn can be referred after appropriate treatment with analgesia, topical antibacterial agent, and possible patching. Minor lid lacerations not involving the lid margin or lacrimal apparatus may be treated and referred.
It is important to emphasize that pain and loss of visual acuity are two markers that can indicate serious ocular pathology. Many, if not most, patients with these presentations require immediate consultation or referral.8 In addition, if the examiner is concerned about a possible central retinal artery occlusion, immediate consultation should be sought for this true ocular emergency.17 If a patient’s eye has been exposed to a chemical or toxic substance, immediate treatment is mandated. Irrigation in the pre-hospital setting should be initiated. When the patient arrives in the ED, the irrigation should be continued and there should be immediate consultation or referral.18 If the EP has any doubts whether the ocular emergency patient can be treated and released, it is better to err by calling a consultant. It must be repeated: With acute vision loss or a change in vision, most cases should be expeditiously evaluated by an ophthalmologist.
With any history of trauma, the physical exam should be buttressed by careful palpation of the bony orbital rim and evaluation for fracture or foreign body presence by ancillary plain films or computed tomography (CT) evaluation.19,20 One must protect the possibly "open eye" caused by blunt trauma or laceration with a secure shield to prevent unintended further damage and loss of ocular contents.21,22 Presence of blood in the anterior chamber warrants ophthalmology consult/follow up.23 With any presentation of pediatric ocular trauma, the emergency clinician should consider the possibility of child abuse. Forty percent of child abuse cases have some ocular manifestations.24,25
Many less serious ocular conditions may require follow up by an ophthalmologist. A number of legal cases could have been avoided with appropriate ophthalmology follow up. Many ophthalmology groups, in cooperation with the ED, reserve an early morning time slot in their offices to re-evaluate the patient. This plan may avoid unnecessary late night calls to the ophthalmologist and affords the patient next day consultation with no hassles with appointment desks, insurance considerations, or other misunderstandings that have caused several successful plaintiff cases.
The unfortunate reality is that many EDs must rapidly move patients through their facilities. The ocular history and physical exam often is incompletely documented. Many EDs have examination formats with check boxes for ocular history and physical examination that can be useful to keep the practitioner on track. Dictation of charts is optimal and expensive, but not universally available.
Discharge Planning
The EP and staff may communicate verbally with patients their diagnoses, treatment plans, and referrals. But unless that information is recorded, any lawsuit that may arise probably will devolve, in part, to a swearing contest about what information was conveyed. Most patients remember details to a degree one would never imagine, and this is because they have only one visit to the provider to recall. Not surprisingly, no EP or nurse can be expected to remember discussions with a patient a year or more after the event, especially after thousands of encounters have occurred since. Customary or standard practice of the EP will be important, as most can advise "what I would have said or done" in the usual course of treatment.
Optimally, the EP should document in the chart and give the patient written information involving the diagnosis, treatment plan, and follow up. Warning signs such as vision changes, increasing erythema or purulence, new onset pain, or exacerbation of pain unrelieved by appropriate analgesics should be a part of the discharge instructions. It is strongly recommended that EDs have ophthalmologic form handouts available at discharge similar to commonly used suture instruction sheets. See Table 4 for an example of discharge instructions.
The coverage for patients who have need for ophthalmology consultation and follow up needs to be addressed by ED management in anticipation of possible problems. There are many issues that may effect ophthalmologic consultation. For example, itinerant eye surgeons from outside the area (perhaps hundreds of miles distant) perform surgery, but are sometimes not available to EPs for consultation. Even local ophthalmologists often have outpatient, non-hospital-based practices. What does an EP do with a patient who has an urgent problem? Optimally, the ophthalmologist should have prior arrangements made for coverage. If not, the consulting staff of the hospital should be involved to ensure coverage and continuity of care. It is recommended strongly that the hospital ED committee plan for these contingencies.
At major emergency centers, proper coverage usually is arranged in advance by the large numbers of ophthalmologists who use the hospital. Small EDs, where no ophthalmologist is geographically near, may have situations arise that produce the greatest exposure. Many ophthalmologists visit small town hospitals, outpatient facilities, or satellite offices a half-day or so a week. It is important for EPs, the department, and the staff of the hospital to communicate with these physicians or other physicians who will be available and willing to take care of patients who are in need of consultation. The key is advance preparation.
Although many EPs have full residencies in emergency medicine, family practice, internal medicine, or other areas that involve evaluation of a variety of presentations, there are many providers who have minimal training and exposure in the ophthalmology area. Additionally, many physician extenders, such as nurses, physician assistants, and family nurse clinicians, may have even greater deficits of experience and training. In a situation involving a provider with limited experience, consultation with an ophthalmologist regarding ocular emergencies should be made as soon as possible if there is any question regarding significant pathology. The minimally trained provider in the ED should not be placed in the position of making a decision that potentially could result in a loss of vision. When in doubt, the provider should err on the side of consultation.
The goal of ED ocular emergency care should be to provide and document appropriate care for the patient under the circumstances. The guidelines provided in this article should be useful to aid the emergency practitioner in preventing or prevailing in any litigation that may occur as a result of the evaluation and treatment of ocular emergencies.
Failure to Follow Up/Document
On March 6, 1994, a 2-year-old patient was brought to the emergency room at Rush Norris Shore with a complaint of something in the eye. The EP diagnosed corneal abrasion and phoned the on-call ophthalmologist, who prescribed antibiotic ointment and recommended that the child be brought to the office the following day. In the lawsuit, the child’s mother claimed she called the ophthalmologist’s office the next day but was advised that, because of insurance reasons, her child would not be seen. The mother claimed the EP gave confusing directions and that she was under the impression she could call the ophthalmologist the next day. The child ultimately was brought to a pediatrician who diagnosed a corneal ulcer, and the child was thereafter treated. The child sustained a corneal scar, depravation amblyopia, and legal blindness in the right eye. The plaintiff claimed the lost vision was the responsibility of the EP. The defendant EP contended instructions were clear and the child was to be seen by an ophthalmologist the following day. As well, the EP denied the eye was infected at the time of the EP’s evaluation, which occurred only two hours after eye injury. The action resulted in a defense verdict for all defendants; however, before trial the ophthalmology group settled for $1 million.26 This case illustrates a number of key areas that help the EP in the assessment of pediatric patients, documentation, and follow-up care.
The importance of an adequate evaluation of an ocular problem in a 2-year-old patient is obvious. On many occasions, the history is not clear and the best an EP can do is thoroughly examine the patient, who usually is uncooperative, crying, and scared. The examination should be orderly, as previously described, with an attempt at visual acuity and observation of the patient’s lids, cornea, and sclera, and an internal eye examination. Most often, these patients may not allow much more than a quick fundoscopic evaluation, when it may be possible to see whether the anterior chamber is clear and red reflex is present. Presence of a red reflex shows that the vitreous and media are clear. The patient’s lids need to be everted to observe whether there is or is not a foreign body present. Staining with fluoresceine is mandatory and, if the patient cooperates, a slit lamp exam would be optimal. With the benefit of a loop, the EP generally can observe corneal abrasions, particularly if they have been stained with fluoresceine. The examiner must be cautious that the staining pattern is one of a foreign body and not one that is indicative of dendritic form. Any evidence of anterior chamber depth change, pupillary movement/irregularities, or extraocular movement differences should be evaluated carefully.
In this particular case, the EP wisely made a call to an ophthalmologist for follow-up, and apparently was able to prove that he referred the patient and gave specific instructions to see the ophthalmologist the next day. The fairly simple treatment in this case and the follow-up to ensure that this patient did not have a chronic problem stemming from acute injury was potentially the most important aspect of this case. Unfortunately, in this situation, the ophthalmologist’s office, because of "insurance reasons," did not see the child promptly. As a result, the child later was seen by a pediatrician and thereafter treated for a chronic corneal ulcer that resulted in permanent vision loss.
This case has importance because the EP was found not to have violated the standard of care. A reasonable evaluation, a consultation, and contact with the follow-up caregiver all helped this EP prove he met the standard of care. Although we do not know the details of why the ophthalmology group settled, one can image the assertion that the patient was not seen for financial reasons was an accelerant in this case and caused the defense to believe that the case at trial was far more dangerous than the settlement of $1 million. If faced with a situation in the ED that involves insurance consideration, it should always be remembered that an EP should treat the patient first and not inquire in any way about the patient’s ability to pay. In many cases, questions regarding ability to pay seem to be one of the key factors that can move a patient with a bad result following treatment to seek legal representation.
Foreign Body
A 33-year-old man was hammering on the U-joint of a car and felt a piece of metal go into his eye. His family doctor recorded spots in vision and sent him to a regional health center to rule out intraocular foreign body. When he presented to the EP, the physician taking the history recorded the patient’s feeling a piece of metal going into the eye, but diagnosed a corneal abrasion. The EP failed to order a CT scan or x-ray to rule out the presence of an intraocular foreign body. The plaintiff was discharged with an eye patch and told to return the following evening if there were problems. Seven months later, the plaintiff noted decreased vision and saw an ophthalmologist whose evaluation showed full retinal detachment with a loss of vision in the affected eye. The case was settled for $250,000.27
This case illustrates a lack of response to a fairly straightforward situation that faces many EP caregivers. The physician attending a patient with a history of metal to metal contact, who also reports "feeling a piece of metal going into the eye," did not rule out an intraocular foreign body.
The local family doctor, who saw the patient first, documents visual acuity changes, perhaps due to lens injury, vitreous injury, or even early retinal tear or detachment. Unfortunately, the evaluation by the EP apparently was never extended beyond the obvious corneal abrasion. It is an absolute need to determine whether corneal abrasion from trauma is deep and whether a foreign body has made that abrasion. There is always the possibility that the patient may have multiple mechanisms of injury with a foreign body actually entering via a different site on the globe and an EP should not be distracted by an obvious corneal abrasion.
This case represents a failure to recognize the historical importance of a metal on metal contact, the need for a complete ocular evaluation with a potential foreign body, and the use of objective modalities to determine whether there is an intraocular foreign body. Often the patient with intraocular foreign body will not present with visual change.
The need to consult an ophthalmologist to discuss the patient with a potential intraocular foreign body at the time of evaluation in the ED is mandatory. These patients can, due to the mechanical or infective nature of the foreign bodies, suffer from a variety of derangements, including lens disruption, vitreous hemorrhage, retinal tears/detachments, and infection leading to total loss of globe.
The case described above probably was indefensible, and a decision was made to settle. It always is arguable that the resulting eye loss probably was going to happen regardless of care. This is a defense that could have been used if this patient had had appropriate, documented consultation. Unfortunately, since there was no consultation, the defense of lack of causation could not be used. Nor could the defense of shared responsibility or consultant responsibility have been used since a consultation was never made.
Failure to Diagnose Orbital Floor Fracture
A 5-year-old was seen by the defendant EP Jan. 30-31, 1992, with complaints of left eye pain after wrestling with an older brother. The EP diagnosed corneal abrasion confirmed by fluorescein dye test. Five months later, the plaintiff’s parents noticed that the child’s left eye, with upward gaze, was not moving to the same extent as the right eye. An orbital floor fracture was diagnosed. The healed fracture site was surgically re-broken and scar tissue formed around the eye muscle. The delay in diagnosis was alleged to be the cause of the movement restriction with double vision when the plaintiff used his eyes in upward gaze. The defendant EP claimed that no classic sign of orbital fracture had been present, including ecchymosis, swelling, numbness, or history of being hit with an object. It also was claimed that the delay in diagnosis and repair did not change the outcome. The jury found in favor of the plaintiff for $125,000.28
This case represents a situation of pediatric ocular injury that has relevance to many ED presentations. The evaluation of any pediatric patient by the EP is difficult. Given the history of left eye pain following wrestling, an eye exam indicating corneal abrasion with conformation by fluorescein dye test seems to be reasonable. However, knowing retrospectively that this patient had an orbital floor fracture, it is apparent that this particular patient probably had an incomplete evaluation of his extraocular movements (EOMs). The patient may not have been able to advise the examiner of double vision or he may not have had it at the time. Usually the diplopia occurs only after the swelling and ecchymosis recedes when the entrapment physiologically occurs. It is important to note in all patients who have potential trauma whether the EOM exam is normal in all extremes. Patients may not realize they have double vision unless asked to move their eyes to extreme gaze directions. Further, pediatric patients with eye injuries should probably be referred for follow up evaluation after their pain has abated.
As is indicated in this summary, the defendant EP advised no classic signs of orbital fracture, including ecchymosis, swelling, numbness, or history of being directly hit with an object (other than a history of "wrestling" with an older brother). Physical exams sometimes are not classic in this regard.
Failure to Diagnose Herpes Keratitis
A 29-year-old presented to a community health care center with complaints of his right eye being red, swollen, watery and with hazy vision. The defendant, a physician’s assistant, diagnosed conjunctivitis and prescribed antibiotic eye drops. Two weeks later, the patient awoke with increased blurred vision. The plaintiff saw an ophthalmologist who diagnosed herpes keratitis, which caused a significant corneal ulcer and permanent visual acuity problems. The plaintiff alleged failure to diagnose herpes keratitis. The defendant contended that as a physician’s assistant, he should not be held to the same standard of care as a physician. The jury returned a $600,000 verdict for the plaintiff.29
This case illustrates a number of potential problems that can occur in the evaluation of patients who visit the ED facility. In this particular case, a physician’s assistant diagnosed conjunctivitis, and gave a prescription of antibiotic eye drops. This situation did not involve a hands-on evaluation by a physician. In today’s practice, physician extenders are used in many ED facilities. Many of these providers are well trained, but some, unfortunately, do not have experience in or understanding of some areas of practice.
In a community health center or an ED, when a patient presents with a red eye, the patient must be evaluated for acute red eye causes, particularly with complaints of "hazy vision" or changes in vision. These complaints usually are not associated with bacterial/viral or allergic conjunctivitis and may be symptoms of corneal disease. However, many of the causes of red eye are benign and will respond to simple antibiotic drop administration.
In this particular situation, it is probable that a fluorescein stain was not used. One might suggest that the patient may have had a bacterial conjunctivitis and later may have acquired the herpetic process. Had the defendant documented a standard ophthalmologic exam including fluorescein stain with negative results, this defensive posture may have been helpful. Because this patient has permanent loss of visual acuity due to herpes keratitis ulcer, there was a significant medical malpractice claim.
The defendant contended that a physician’s assistant should not be held to the same standard of care as a physician. This was probably a contentious issue. A physician’s assistant must work within the standard of care of physician’s assistants. However, the standard of care attributed to the physician’s assistant should be no lower than that of the attending physician or the physician who has signed off on the protocols followed by the provider. It is dangerous to assert that because a patient is seeing a physician’s assistant, he should expect a lower standard of care than if a physician was evaluating him.
A better rule to follow within the ED relative to the evaluation, diagnosis, and treatment by a physician extender involves asking a physician to review the patient’s clinical picture if there are key historical/physical findings compatible with vision threatening conditions, e.g., pain and changed vision. Charts should be reviewed before the patient exits the department and the EP should cosign the completed chart. Lack of chart review is a common problem in large centers with medical students/ interns/residents. These providers should always be closely evaluated by EPs and their charts cosigned. The EP always should see a patient who has a potentially significant ophthalmologic disorder.
Ophthalmology Telephone Consult
On Aug. 31, 1991, an infant was brought to the ED following a fishing accident-induced eye injury. A physician’s assistant first saw and examined the infant. The patient was examined by an EP who contacted an ophthalmologist. He described a hyphema that was involving the inferior half of the anterior chamber. The ophthalmologist questioned and advised the EP over the phone, but did not want to examine the infant. The child was given a prescription for eye drops and told to take over-the-counter agents for pain. There was no direct contact by the ophthalmologist with the patient. All caregivers were sued for standard of care violations involving failure to immediately have an ophthalmology specialist see and treat the patient. Because of the delayed evaluation, the patient lost his eye and all providers contributed to a settlement after the appeal process, even though there was testimony that a better outcome was not probable.
At trial, the ophthalmologist contended that he had been on courtesy/consulting staff at the hospital for many years and answered questions for the ED staff over the phone, but did not ever see patients at the ED and did not receive payments for any courtesy consultation. He advised that he rendered an informal opinion over the phone and since he did not see, examine, take a history from, or treat the child, he was not responsible for the patient. The ophthalmologist testified that he did not feel it necessary to see the child due to his comfort with the EP’s responses to his recommendations.30
This case represents the prevailing opinion that a physician’s giving of advice over the phone may furnish sufficient basis upon which to conclude that there is a implied physician-patient relationship. If a call in this matter advises the prospective patient of the course of treatment, it is foreseeable that the patient would rely upon the advice.
It is important to understand that the ophthalmology defendant in this case apparently was apprised of a history and physical examination and did conclude that certain treatments as described were indicated. In a similar circumstance, an EP must be careful giving any advice over the telephone to patients or family who may call. The general rule is to not give advice by telephone because of the absolute need to evaluate the patient’s problem in person in the controlled environment of the ED. The EP, by the ophthalmology consultation, met the standard of care and was a conduit for the ophthalmologist’s physician-patient relationship.
Foreign Body and Comparative Fault
A patient was working as an automobile mechanic and was injured when a foreign body entered his right eye. He sought treatment immediately and was examined by the attending EP, who inserted several drops in his right eye and prescribed an eye patch. The EP did not take an x-ray, nor did he examine the eye with any mechanical instruments other than a flashlight. The examination revealed that although the eye was scratched, the EP did not detect the presence of a foreign object in the eye. He advised the plaintiff to apply drops in his right eye four times a day and assured him the scratch would heal.
Over the next several months, the plaintiff experienced headaches and tearing and noticed his eye became sensitive to light. Within four months, his vision in his right eye had deteriorated and was impaired so much that he could not drive. He was referred to an ophthalmologist at that time and his condition was diagnosed as retinal detachment, corneal ulceration, and an intraocular foreign body. The patient was treated for 10 days before a surgical procedure by a retinal surgeon was performed to remove the foreign object and treat the retinal detachment. He had a nine-month recovery.
A trial jury found that plaintiff suffered damages of $809,000 and found the EP 60% at fault and the ophthalmologist 40% at fault. Upon appeal, the ophthalmologist was able to assert successfully that there was no proof that medical treatment rendered by him fell short of the standard of care or that his treatment proximally caused the plaintiff’s injuries.31
This case illustrates another significant standard of care issue relative to a patient having a strong history of foreign body intraocular injury without adequate exam and documentation. The EP directed no consultation or follow up, and as a result, a period of months passed before appropriate medical care was given.
It is of interest that the jury believed that the ophthalmologist was 40% liable for the total sustained monetary damages. Comparative fault is used in many states to assign liability by specific percentage to defendants who have been proven to have liability. In most states, the plaintiff can be to have some degree of fault, and in some states, if the plaintiff has greater than 50% fault, the plaintiff cannot recover. [Editor’s note: It’s interesting how this patient’s symptoms got progressively worse, yet he did not arrange follow-up or return to the ED. Patients need to be accountable for their actions (or, in this case, inactions), as well. Apparently, the jury in this case did not buy into that argument.]
In this particular case, an unfortunate lack of attention to the basic history and necessary physical exam certainly played a part in this EP’s exposure. The ophthalmologist as a defendant was excused, since the alleged delay in referral to a retinal surgeon was not causative of the ultimate eye damage.
Improper Treatment of Corneal Ulcer and Failure to Follow Advice, with Resultant Legal Blindness
The plaintiff, a 29-year-old patient, went to an urgent care clinic and was treated by the defendant EP for a severe infection of the right eye with suspected corneal ulcer. The plaintiff was referred to an ophthalmologist, but did not go. On the same evening, she was seen by physicians at a local hospital and again was diagnosed as having a severe eye infection with corneal ulcer. The patient returned to the hospital the following day and saw another physician, who referred her to an ophthalmologist whose diagnosis was conjunctivitis with corneal ulcer.
The plaintiff asserted that as a result of improper treatment of her corneal ulcer she became legally blind. The defendant EP asserted that he scheduled an appointment for the plaintiff the same day the patient was seen in the ED. The jury returned a unanimous verdict for the defendant.32
This case illustrates that patients may not follow advice, and this lack of follow up can result in injury. The patient from this case description was a person who, unfortunately, would not immediately see an ophthalmologist. The EP appropriately made his evaluation and referred this patient with significant infection and ulcer to an ophthalmologist. His documentation apparently was appropriate and his testimony was believed by the jury.
There is no question that communication with patients in the ED setting is difficult. Patients often do not have the ability to understand their disease process. Occasionally, they do not have the emotional or mental stability to make judgments about follow up care. It is a necessity to document what advice is given to these patients and to do everything possible to ensure anyone with the patient is told of treatment plans and referrals.
The system failure in this particular case was not the EP’s fault. This case could be categorized as an "against medical advice" case where the patient is given every opportunity to gain appropriate treatment, but does not follow advice. It is difficult for plaintiffs to win these types of cases, but it is necessary for the EP and/or other health care providers to go the extra mile to make sure that an informed decision relative to refusal of care is made.
Conclusion
Each of these legal cases points out failures in multiple areas of care. Although the EP was the defendant in each, it is reassuring to understand that the EP usually can prevail with appropriate care and documentation regardless of the allegation of the plaintiff. Unfortunately, some cases reflect the absence of attention to detail, as it is detailed in the case analysis, that superficial evaluations lead to liability. Patients often have less than favorable results form their ocular disease process or injury. The EP must clearly communicate with the patients, the consultant if needed, and in the chart to prevent becoming an unsuccessful defendant should a medical malpractice action be brought involving care.
Endnotes
1. Harvey J. Introduction to orbital disease. In: Duane’s Clinical Ophthalmology, Vol. 2. Philadelphia: Lippincott-Raven; 1996.
2. Catalano RA. Examination of the eye. In: Ocular Emergencies. Philadelphia: WB Saunders; 1992: 3-43.
3. Clark RB, Farber JM, Sher NA. Eye emergencies and urgencies. Patient Care 1989;23:24-42.
4. Erie JE. Ophthalmic history and examination. In: Bartley GB, Liesegang TJ, eds. Essentials of Ophthalmology. Philadelphia: JB Lippincott; 1992:3-25.
5. Friedberg MA, Rapuano CJ. Trauma. In: Wills Eye Hospital-Office and Emergency Room Diagnosis and Treatment of Eye Disease. Philadelphia: JB Lippincott; 1990:17-45.
6. Tasman W, Jeager EA, eds. Systemic ophthalmology. Duane’s Clinical Ophthalmology, Vol. 5. Philadelphia: Lippincott-Raven;1996.
7. Rothenhous TC, Polis MA. Ocular manifestations of systemic disease. Emerg Med Clin North Am 1995;13:607-630.
8. Parrish CM, O’Day DM. Herpes simplex keratitis. Duane’s Clinical Ophthalmology Vol. 4. Philadelphia: Lippincott-Raven; 1996.
9. Brunette D, Ghezzi K, Renner G. Ophthalmologic disorders. Rosen P, ed. Emergency Medicine, 4th ed. St. Louis: Mosby-Year Book Inc.;1998:2698-2718.
10. Catalano RA. Examination of the eye. Ocular Emergencies. Philadelphia: WB Saunders; 1992:130,190.
11. Deutsch TA, Feller DB. Management of Ocular Injuries. Philadelphia: W.B. Saunders; 1985.
12. Newell FW. Ophthalmology Principles and Concepts. 8th ed. St. Louis: Mosby; 1996.
13. Clark R. Ocular emergencies. In: Fartinalli JE, Krome RL, Ruiz E, eds. Emergency Medicine: A Comprehensive Study Guide. 3rd ed. New York: McGraw-Hill; 1992:834.
14. Barish RA, Naradzay J. Ophthalmic therapeutics. Emerg Med Clin North Am 1995;13:649-667.
15. Coster DJ. Superficial keratopathy. Duane’s Clinical Ophthalmology, Vol. 4. Philadelphia: Lippincott-Raven; 1996.
16. Petroutsos G, Guinaraes R, Gorand J, et al. No eye pad for corneal abrasion. Eye 1993;7:468-471.
17. Kathol RG, Cox TA, Corbett IJ, et al. Functional visual loss. Arch Ophthalmic 1983;101:729-735.
18. Heyrih SS, Kolder H, Weingeist TA. Central retinal artery occlusion and retinal tolerance time. Ophthalmology 1980; 87:75.
19. Ralph RA, Slansky HH. Therapy of chemical burns. Int Ophthalmol Clin 1974;14:17.
20. Wilkins RB, Harris WE. Current treatment of blow out fractures. Ophthalmology 1982;89:464.
21. Smith B, Erguin WF Jr. Blowout fracture of the orbit: Mechanism and correction of internal orbital fracture. Am J Ophthalmol 1957;44:733.
22. Mathog RH. Basic management of soft tissue injury. In: Spoon TC, Nesi FA, eds. Management of Ocular, Orbital, Adnexal Trauma. New York: Raven Press; 1998:365-379.
23. Holt JE, Holt GR, Blodgett JM. Ocular injuries sustained during blunt facial trauma. Ophthalmology 1983;90:14-18.
24. Rubin SE, Catalano RA. Ocular trauma and its prevention. In: Nelson LB (ed). Harley’s Pediatric Ophthalmology. Philadelphia: W.B. Saunders Co.; 1998:482-498.
25. Kiffrey GT. The eye of the battered child. Arch Ophthalmology 1964;72:231.
26. Farrell Loebbaka, minor v. Dr. Kelly Asperheim, MD, Rush North Shore Hospital, Emergency Physician’s Group Ltd., d/b/a EPG Ltd. Cook County (IL) Circuit Court, Case No. 95L-3479. June, 2000.
27. David Claxton v. Janet Jordan, Greene County (MO) Circuit Court, Case No. 196CC2885. July 1998.
28. Kevin Gaughan v. Robert Gibula, MD, SC McHenry Co. (IL) Circuit Court, Case No. 94L-22. March, 2000.
29. Jeffrey Miller v. Jerry Feuer, P.A. and Fenway Community Health Center, Inc., Suffolk County (MA) Superior Court, Case No. SUCV1998-00448-C. March, 2002.
30. Gregory Cogswell, an Infant, by Donald W. Cogswell, et al., His Parents and Guardians, Respondent, vs. Glen Chapman, et al., Respondents, and William Eichner, Doing Business as Eye Care Associates, Appellant. 249 A.D.2d 865, 672 N.Y.S.2d 460. April 30, 1998.
31. Carmine Foresta, Respondent, et al., Plaintiff, v. Makram Armanios Tadros, Appellant, et al., Defendants (and a third-party action). 164 A.D.2d 904, 559 N.Y.S.2d 578. Aug. 20, 1990.
32. Colette Jones v. Duane W. Dodd, MD, Michael Brinkenhoff, MD, and Ventura County Medical Center, Ventura County (CA) Superior Court, Case No. SC 019487. Oct. 2000.
The emergency physician (EP) and nurse often may encounter patients with the chief complaint of eye pain or visual problems. Generally, the diagnosis easily is obtained and quickly treated. Unfortunately, a subset of patients will present with an illness that threatens permanent vision loss or impairment. EPs must have a broad differential diagnosis and structured approach in evaluating these patients to ensure appropriate diagnosis and treatment.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.