ECG Review - Mobitz I or Mobitz II AV Block?
ECG Review
Mobitz I or Mobitz II AV Block?
By Ken Grauer, MD, Professor Emeritus in Family Medicine, College of Medicine, University of Florida
Dr. Grauer is the sole proprietor of KG-EKG Press, and publisher of an ECG pocket brain book.
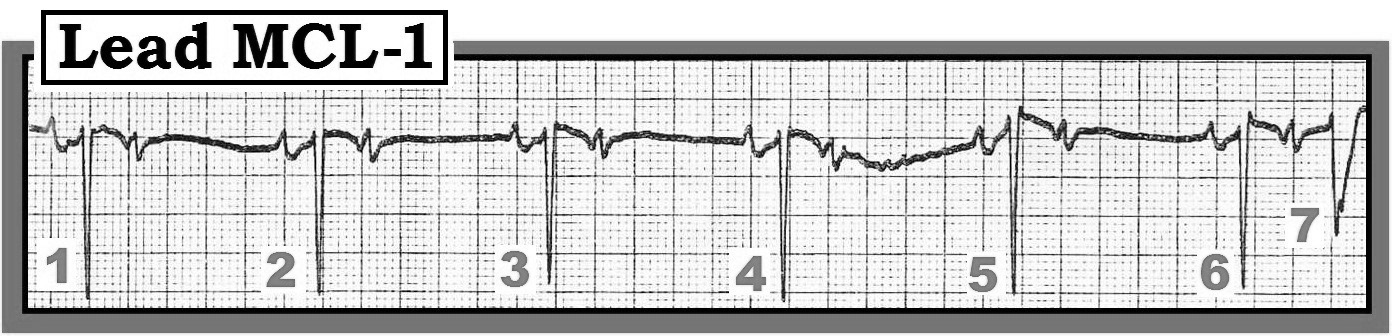
Figure — Lead MCL-1 rhythm strip. Is this Mobitz I or Mobitz II?
Scenario: Interpret the lead MCL-1 rhythm strip shown in the figure. Does this rhythm represent Mobitz I (Wenckebach) or Mobitz II AV block? Is a pacemaker likely to be needed?
Interpretation: Neither Mobitz I nor Mobitz II is present. Rather than AV block, the rhythm in the figure represents an insightful example of the "mischief" that blocked premature atrial contractions (PACs) can cause, especially when PACs are frequent.
All forms of AV block are characterized by the presence of similar morphology P waves that occur with a regular (or at least fairly regular) P-P interval. Requiring similar P wave morphology when assessing an arrhythmia for AV block eliminates other potential causes of bradycardia such as wandering pacemaker, sinus pauses, and sinus arrest. So while occasional PACs with differing P wave morphology may be seen, the presence of constantly changing P wave morphology should suggest some phenomenon other than AV block.
With regard to regularity of the atrial rate, slight variation in the P-P interval may be seen with AV block when there is underlying sinus arrhythmia. However, gross variation in the P-P interval is usually not seen when the primary problem is AV block.
Keeping these two points in mind allows us to rule out AV block as the cause of the rhythm disturbance in the figure. The P-P interval is clearly irregular. In fact, there is a pattern to this P-P variation (alternating short-long cycles) produced by the finding that every other P wave is early (premature). The underlying rhythm is atrial bigeminy (every other beat is a PAC). In addition, P wave morphology changes from one beat to the next. Sinus P waves are seen as a biphasic (positive-then-negative) deflection preceding beats 1, 2, 3, 4, 5, and 6. In contrast, P waves buried within the ST-T wave of beats 1 through 6 are triphasic (small negative, then positive, then narrow negative), deflections that clearly look different in morphology than the sinus P waves. These triphasic P waves arise from an atrial site other than the sinus node.
In summary, the underlying rhythm in the figure is atrial bigeminy. The very early occurring PACs (buried within the T waves of beats 1 through 5) are non-conducted because they occur during the absolute refractory period. In contrast, the PAC that occurs within the T wave of beat 6 is conducted, albeit with aberration (because it presumably occurs during the relative refractory period). No AV block is present. No pacemaker is needed. Clinically, blocked PACs are much more common than any form of heart block. They may be recognized by careful attention to P wave regularity, morphology, and careful search for the "telltale" notching of a hidden PAC within T waves preceding a relative pause on the tracing.
For more information on the basics of AV block, please visit: https://www.kg-ekgpress.com/av_block_pdf_file/.
Subscribe Now for Access
You have reached your article limit for the month. We hope you found our articles both enjoyable and insightful. For information on new subscriptions, product trials, alternative billing arrangements or group and site discounts please call 800-688-2421. We look forward to having you as a long-term member of the Relias Media community.