By Ken Grauer, MD
Professor Emeritus in Family Medicine, College of Medicine, University of Florida
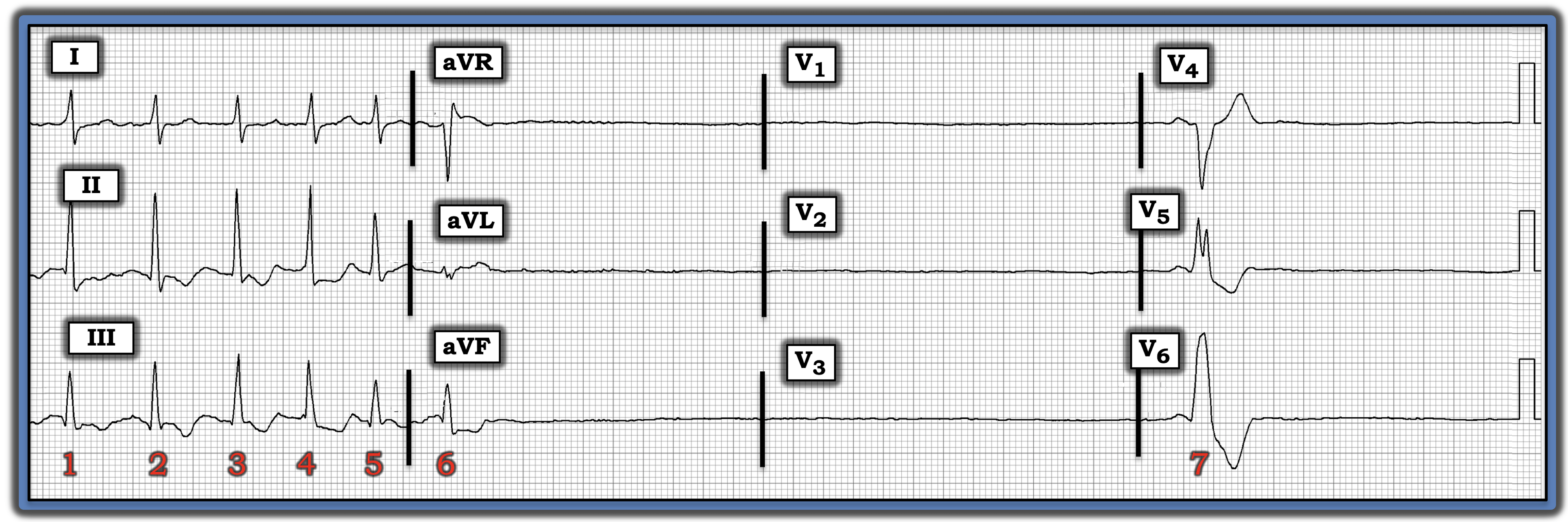
The ECG in the figure is from an older woman who complained of a number of short-lived “episodes” beginning the day this tracing was recorded.
• Note: This is not a rhythm strip. Instead, it is a 12-lead ECG.
• How would you interpret this tracing? What is this patient’s probable diagnosis?
Interpretation: The ECG in the figure begins with six narrow, rapidly occurring and irregularly irregular QRS complexes, but without any P waves. This description defines these six initial beats as a run of fast atrial fibrillation.
• Immediately following the sixth beat, there is a nearly 5-second pause (i.e., with no QRS complex for a duration of more than 24 large boxes).
• Beat #7 is wide. It is difficult to know if beat #7 represents a ventricular escape beat or a sinus-conducted beat with left bundle branch block because the PR interval before this beat looks to be short. That said, it does not matter clinically whether beat #7 is or is not conducted, since this patient’s underlying problem remains the same.
• Another extended pause of at least 2.0 seconds in duration immediately follows beat #7, before being interrupted by the end of the ECG recording.
Impression: In view of this patient’s older age, it is likely that she has sick sinus syndrome (SSS) and will need a pacemaker.
• SSS is a diagnosis of exclusion to be made only after ruling out potentially “fixable” causes of the rhythm shown in the figure. Among the entities to be ruled out include excessive use of rate-slowing medication, acute ischemia or infarction, hypothyroidism, electrolyte disturbance, and sleep apnea.
• Although the period of monitoring shown in the figure only lasts 10 seconds, we see several characteristic features of SSS. These include intermittent rapid atrial fibrillation, sinus node suppression following tachycardia, and extended pauses with delayed escape beats.
• SSS is by far the most common indication for permanent pacing among older individuals. Although many patients go for years with minimal symptoms, the combination of rapid atrial fibrillation followed by extended pauses makes medical management of today’s patient nearly impossible, since drugs used to control rapid atrial fibrillation will only exacerbate this patient’s bradyarrhythmias.
Note: For more information about and further discussion of this case, please visit: https://tinyurl.com/KG-Blog-342